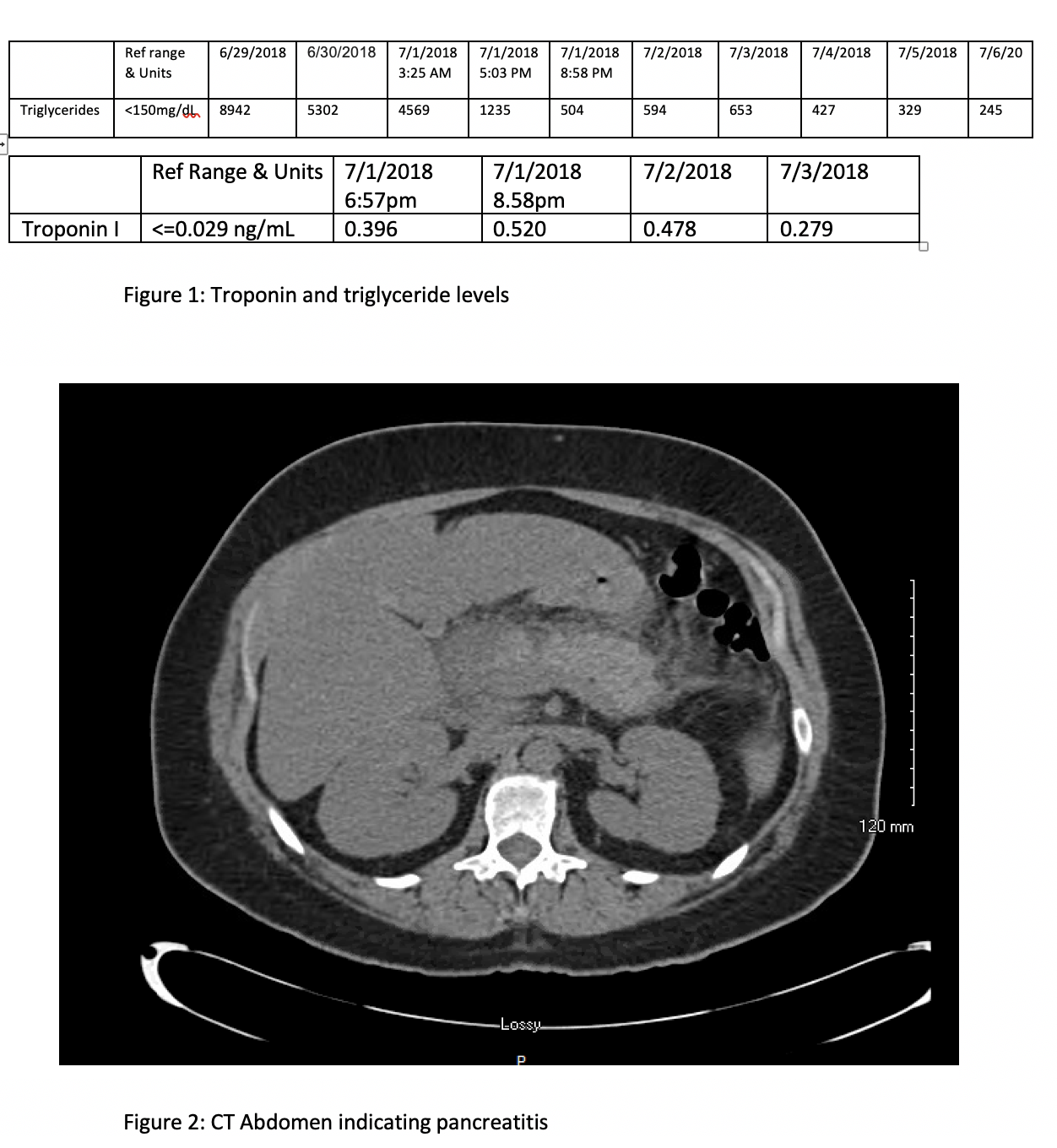
Case Presentation: A 43-year-old Caucasian woman with acute pancreatitis due to familial hypertriglyceridemia was admitted with triglyceride levels of 8942 mg/dl (Fig 1). She had had three past hospitalizations related to the hypertriglyceridemia, including a similar admission for pancreatitis and one for myocardial infarction. While she had previously been prescribed anti-lipemic medications, she had to stop them when she lost her insurance. CT scan of the abdomen/pelvis confirmed acute pancreatitis (Fig 2). She was treated with IV fluids; three sessions of plasmapheresis reduced triglycerides to 245. Unfortunately, she also had positive troponin levels (Fig 1) suggesting NSTEMI, although ECG was negative for acute ischemic changes; she was managed medically with unfractionated heparin. She was discharged on fenofibrate, atorvastatin, gemfibrozil and fish oil.
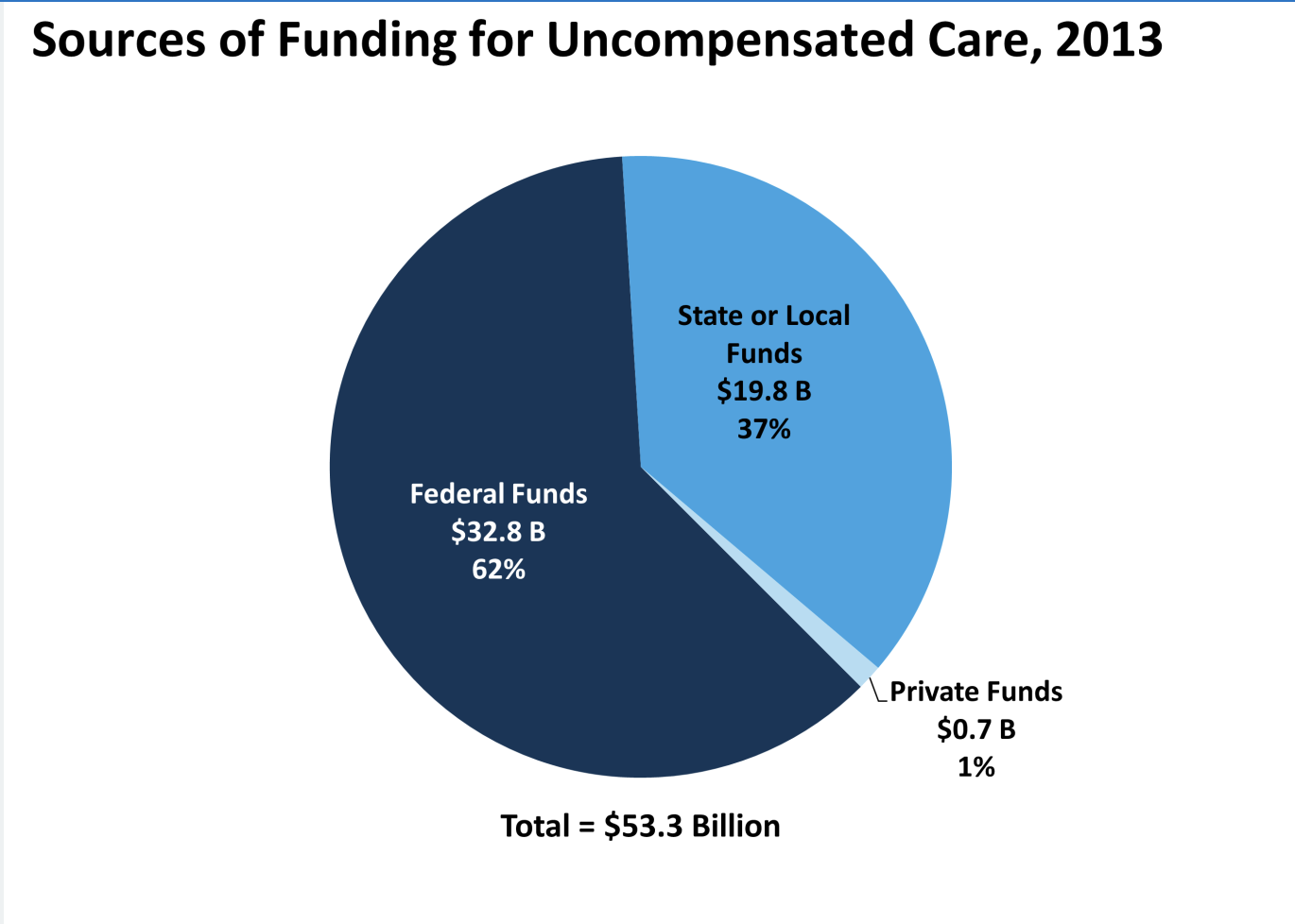
Discussion: One in six Americans under age sixty-five lacks health insurance, imposing sizable hidden costs upon society. We present a case of a 43-year-old uninsured woman with multiple theoretically preventable hospitalizations for hypertriglyceridemia.Millions of uninsured Americans use health care services annually; many cannot pay their medical bills. In 2013, the cost of “uncompensated care” provided to uninsured individuals was $84.9 billion. Uncompensated care includes health care services without a direct source of payment. Uninsured patients also paid an additional $25.8 billion out-of-pocket for care. In 2013, $53.3 billion was paid to help providers offset uncompensated care costs, which mostly came from public dollars (Fig 3). Our patient has had multiple hospitalizations for hypertriglyceridemia due to lack of insurance and inability to afford medications. Her plasmapheresis added to her skyrocketing hospital bill. The cost of 12 months of her anti-lipemic medication is dwarfed by the 6 figure bill for her 10-day hospitalization. Unsurprisingly, one cohort study showed that since uninsured people are less likely to receive continuity of medical care, they have a higher mortality rate compared to those e with employer-provided insurance.
Conclusions: The United States trails many other OECD countries in access to care indicators. Despite an increase in coverage from 85.6% in 2013, it is still not universal, with only 91% of the population covered by insurance (the second lowest coverage rate after Greece). Further, 22% of Americans in 2016 skipped consultations due to cost (compared to an OECD average of 9.1%), and 18% did not purchase prescribed medicines. The access problem is particularly marked for poorer families, with 43% of low-income adults reporting unmet care needs. As our case illustrates, this results in preventable poor medical outcomes and expenses.