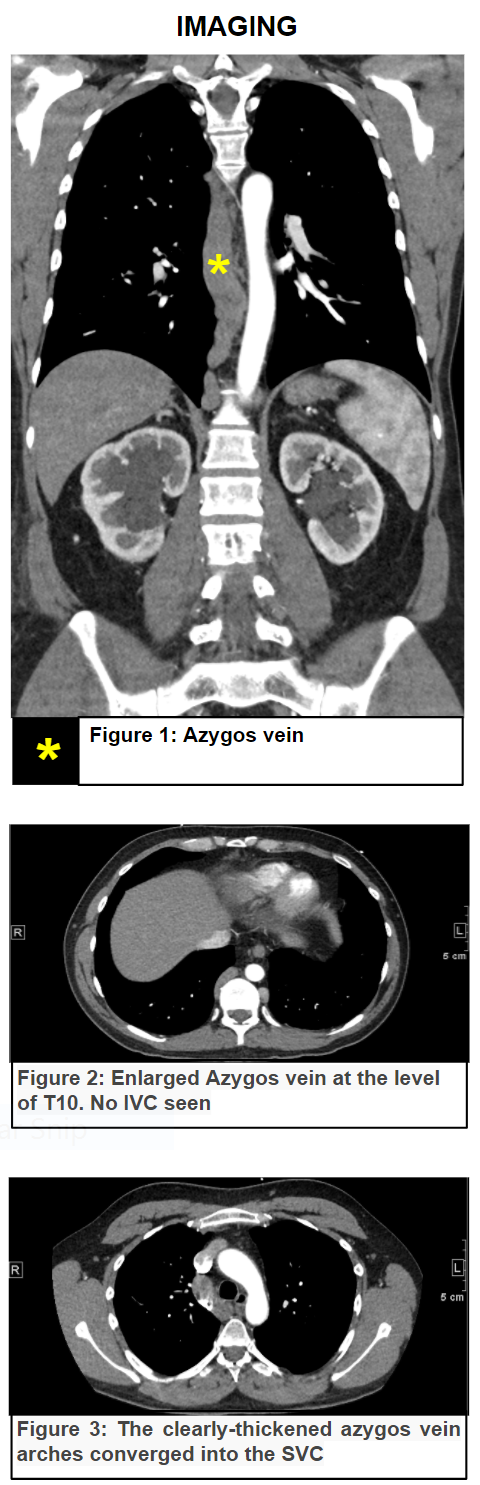
Case Presentation: Azygous continuation, an uncommon vascular anomaly that results from aberrant development during embryogenesis. It occurs in less than 0.6% of the population and may be associated with other congenital abnormalities. In adults aged between 20-40 years, the reported incidence is 10 times lower. With the increased use of different imaging studies such as HCT scan, MRI, and ultrasound these anomalies are being identified more often particularly in asymptomatic patients. Our patient is a 39-year-old gentleman who presented with worsening low back pain, bilateral lower extremity pain and swelling for 10-day duration. He was found to have “unprovoked” bilateral proximal DVT. The patient underwent CT of his chest and abdomen to evaluate his back pain. An Inferior Vena Cava (IVC) agenesis with azygous continuation incidentally discovered. The patient was successfully treated with anticoagulants and EKOS thrombolytic therapy was performed.
Discussion: Azygos continuation (AC) is a rare anomaly caused by the absence of the hepatic part of the IVC with blood flow to the Azygos vein, which joins the SVC in the right paratracheal space.
Some authors have suggested that such congenital abnormalities predispose to DVTs, as the venous system is not adequately able to drain the lower extremities despite the compensatory collaterals. This predisposes to venous stasis and endothelial injury, which are significant risk factors for DVT.
As per our knowledge, only a handful of cases involving bilateral DVTs and azygos continuation have been reported in the literature so far. Formerly, an underlying malignancy was the principal condition associated with bilateral DVT, but it is getting more apparent that congenital anomalies of the IVC should always be kept in mind when investigating young adults with Bilateral DVT with no associated risk factors.
Clues for diagnosis are the presence of extensive and bilateral iliac thrombosis and an enlarged shadow of the azygos vein on chest X-rays. HCT scan and MRI are the gold standard modalities to diagnose IVC anomalies.
DVT management in patients with IVC anomaly must focus on its prevention. For instance, labeling patients with IVC anomalies in the EMR system especially if they were diagnosed incidentally, not to underestimate their presenting symptoms. Other reported cases recommend avoidance of situations that provoke DVT such as inactivity and OCP.
Apart from what’s mentioned above, we recommend periodic Doppler U/S for the LE starting at age of 30, and to perform well designed prospective studies to evaluate the efficacy of prophylactic anticoagulation therapy in young adults with IVC anomalies.
Till now, there is no data to inform on the precise duration of anticoagulation therapy in patients with IVC anomalies presenting with deep vein thrombosis.
Conclusions: IVC agenesis is a rare condition. The physician should suspect this in young patients with extensive “unprovoked” DVT in bilateral lower extremities.