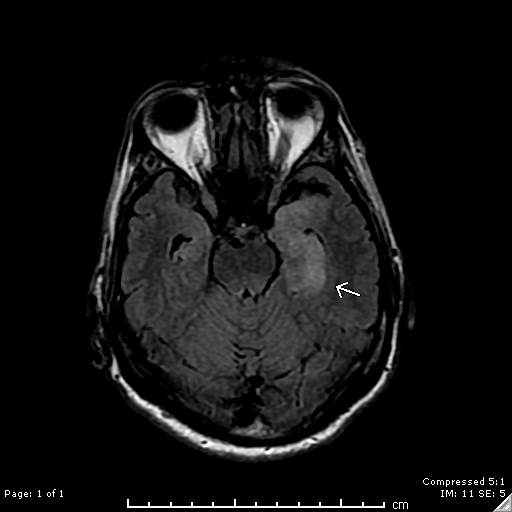
Case Presentation: A 59-year-old male was transported to the emergency department by concerned family and friends who had noted progressive confusion over a 72-hour period. The patient had failed to perform several routine parenting and household duties, and was unable to recognize familiar friends and colleagues. The patient denied fever, headache, and neck discomfort. There was no reported history of alcohol or substance abuse. He denied any at risk behaviors for HIV. Neurological exam was remarkable only for subtle cognitive defects. CAT of the brain was unremarkable. Brain MRI revealed asymmetric edema in the left mesial temporal lobe with restricted diffusion along the hippocampal cortex, suggestive of viral encephalitis (Image 1). Lumbar puncture was performed and demonstrated pleocytosis with CSF RBC of 3,000/uL, and WBC 16/uL with 79% lymphocytes. CSF protein was elevated at 65 mg/dL. Acyclovir was empirically started for presumed herpes encephalitis. Subsequently, HSV Types 1 and 2 PCR testing on the CSF returned as negative, and serum testing for HIV1 antibody returned as positive. HIV1 RNA by PCR was 68,800 copies/mL. Absolute CD4 count was 121/uL. Serum RPR was as positive at 1:128, and reflex antibody testing for Treponema pallidum was positive. CSF VDRL was also positive at 1:4. Treatment with a planned two-week course of ceftriaxone was initiated. The patient will begin anti-viral therapy for HIV as an outpatient.
Discussion: Neurosyphilis is defined as infection of the central nervous system by Treponema pallidum, a spirochete that is transmitted sexually. It is most common in patients infected with HIV. A positive CSF VDRL at any dilution establishes a definitive diagnosis. Described by Sir William Osler as “The Great Imitator”, syphilis can present with a myriad of different clinical manifestations. Less than ten cases of neurosyphilis with signs, symptoms, and imaging findings consistent with herpes simplex encephalitis (PLEDS and hyperintense T2-weighted signals involving the temporal lobe) have been reported in the world literature. Other entities that may rarely present with similar clinical and MRI findings include systemic lupus erythematosus related vasculitis, gliomatosis cerebri, acute hemorrhagic leukoencephalitis, prolonged partial complex seizures, and paraneoplastic limbic encephalopathy. Treatment of choice of neurosyphilis is a prolonged course of intravenous penicillin, with repeat CSF exam at 3 months to assess clearing of pleocytosis and lack of VDRL reactivity.
Conclusions: In the setting of encephalitis with imaging evidence of temporal lobe inflammation, negative HSV antibody testing should prompt expansion of the diagnostic evaluation, and should include serological screening for Treponema pallidum infection.