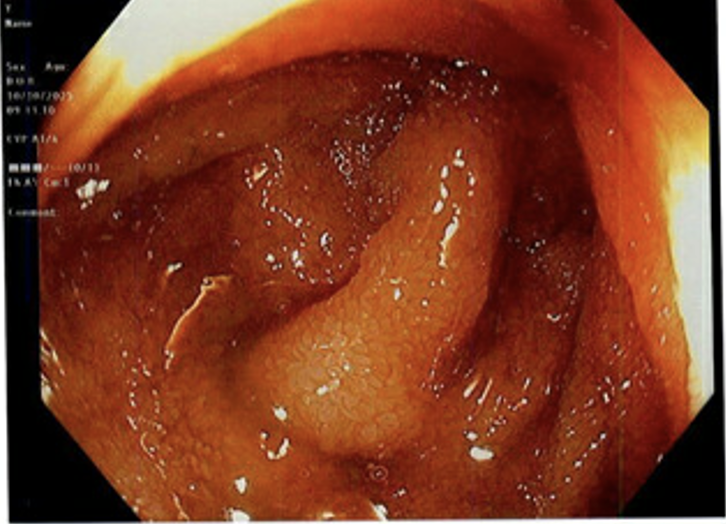
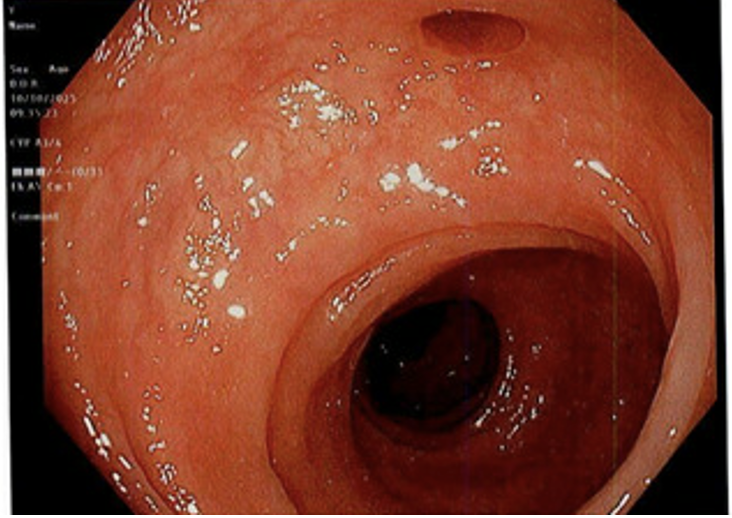
Case Presentation: A 75-year-old woman with past medical history of hyperlipidemia and gastroesophageal reflux disease presented to the hospital in June 2025 after being found by her primary care provider to have a hemoglobin of 6.5 g/dL during routine evaluation. She endorsed progressive fatigue but denied hematemesis, melena, hematochezia, or abdominal pain. Laboratory studies confirmed iron deficiency anemia (ferritin 5.8 ng/mL, transferrin 392 mg/dL, total iron-binding capacity 490 µg/dL). She received two units of packed red blood cells and two doses of intravenous ferumoxytol, with complete recovery of hemoglobin and resolution of symptoms. She remained stable for several months.In October 2025, she presented again to the hospital with fatigue and weakness. Outpatient labs showed hemoglobin 6.0 g/dL, prompting a second admission for recurrent anemia. She continued to deny overt bleeding. Prior endoscopy in 2023 had shown a 5 cm hiatal hernia with mild non-erosive gastritis, and colonoscopy revealed mild diverticulosis, neither of which identified a bleeding source.During this admission, repeat endoscopy demonstrated an enlarging 10 cm hiatal hernia with two small Cameron erosions and short-segment Barrett’s esophagus. Colonoscopy again showed only diverticulosis. Small-bowel follow-through was normal. She received intravenous iron sucrose and one unit of packed red blood cells, with clinical improvement. She was discharged on proton-pump inhibitor therapy with gastroenterology and surgical follow-up arranged.
Discussion: Iron deficiency anemia in older adults is common, but recurrence after complete recovery should prompt reconsideration of the initial diagnosis and prior evaluations. This patient’s first endoscopic workup in 2023 was reassuring; however, a repeat evaluation revealed Cameron lesions within a large hiatal hernia, an uncommon but clinically important source of chronic blood loss.This case demonstrates how diagnostic closure after “normal” studies can delay recognition of subtle structural causes. Cameron lesions often heal intermittently and may be missed if the hernia sac is not carefully inspected. For hospitalists, the key lesson is to maintain diagnostic vigilance and consider structural etiologies when standard workups are unrevealing. Early recognition allows treatment with acid suppression, iron repletion, and, when necessary, surgical repair, preventing repeated transfusions and hospitalizations.
Conclusions: In elderly patients with recurrent iron deficiency anemia after previously normal endoscopic evaluations, Cameron lesions associated with large hiatal hernias should remain an important diagnostic consideration. Although frequently overlooked, Cameron lesions have been reported in 5–9.2% of patients with iron-deficiency anemia, underscoring that they are a more common structural cause than often recognized. Early identification can prevent repeated admissions, unnecessary investigations, and transfusion dependence, improving outcomes for older adults with recurrent anemia.