Background: Traumatic brain injuries (TBIs) pose a unique problem because prognosis is difficult to predict; therefore, treatment decisions are complex with uncertain outcomes. According to the American College of Surgeons 2018 Trauma Quality Improvement Project (TQIP), identified patients should receive a palliative care assessment within 24 hours, a family conversation should be held within 72 hours, and repeated every three to five days.(1) The palliative care service provides support and addresses the needs of the patient and family to improve the quality of life(2), which could benefit these patients.
Methods: This study intends to determine the effect of palliative care consults on outcomes of adult patients with TBIs.This is an IRB exempt retrospective pre-/post-ad hoc analysis using The Pennsylvania Trauma Outcomes Study (PTOS) database. The primary outcome was in-hospital mortality in consulted patients. Secondary endpoints include length of stay (LOS) and hospital cost.
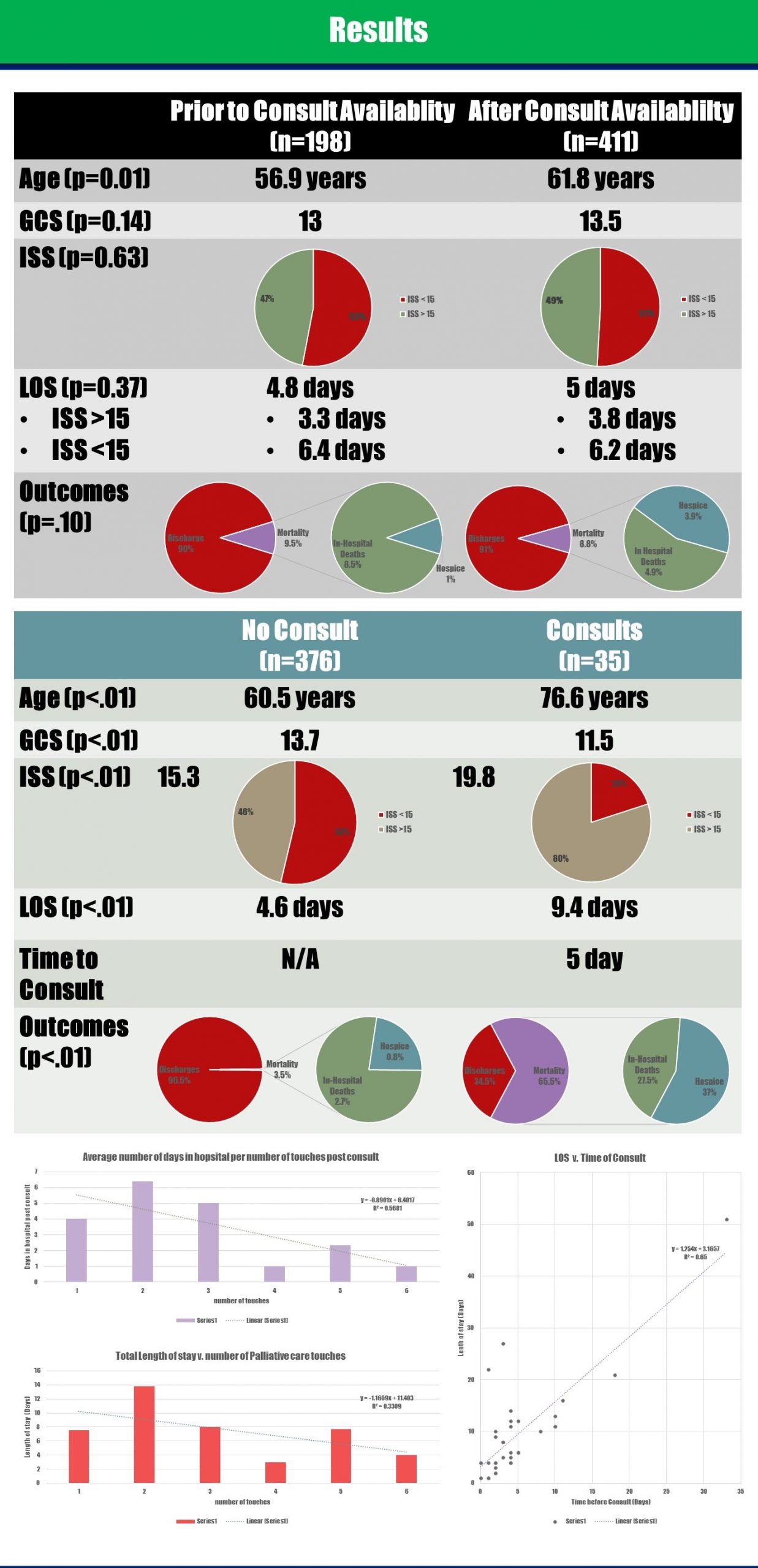
Results: Consulted patients were older and more severely injured with a greater decrease in level of consciousness; a mean age of 76.6 v. 60.5 years (p<0.01), an ISS of 19.8 v. 15.3 (p<0.01), and a GCS of 11.5 v. 13.7 (p<0.01). Average time to consult was 5 days. Consults within 3 days and after 3 days of admission stayed an average 6.4 days and 12.5 days respectively. Increased number of palliative care visits correlated with a decreased LOS. Patient mortality was 9.5% the year prior to consults beginning and 8.8% the years after. The in-patient mortality was 8.5% before the consult service and 4.9% after the consult service became available (p=0.10).
Conclusions: We observed a decrease in in-hospital mortality and an increase in discharges to hospice. We anticipate that palliative care also increases family and patient satisfaction despite outcomes. A literature review showed consults were most effective within 48 hours of admission(3), patient mortality was unchanged(4,5), and LOS could be reduced(3) . The data analyzed was prior to the TQIP publication, and while our time frame did not coincide with the guideline; our results did reflect consistent recognition of an appropriate demographic and suggest earlier and more frequent visits can decrease LOS. If we consistently reduced our time to consult we could reduce patients LOS and save at least $3,184 to $3,968 per day(6). Future steps include a protocol to shorten our time to consult(7) allowing for more visits and assessments of patient satisfaction and hospital cost with a prospective analysis.