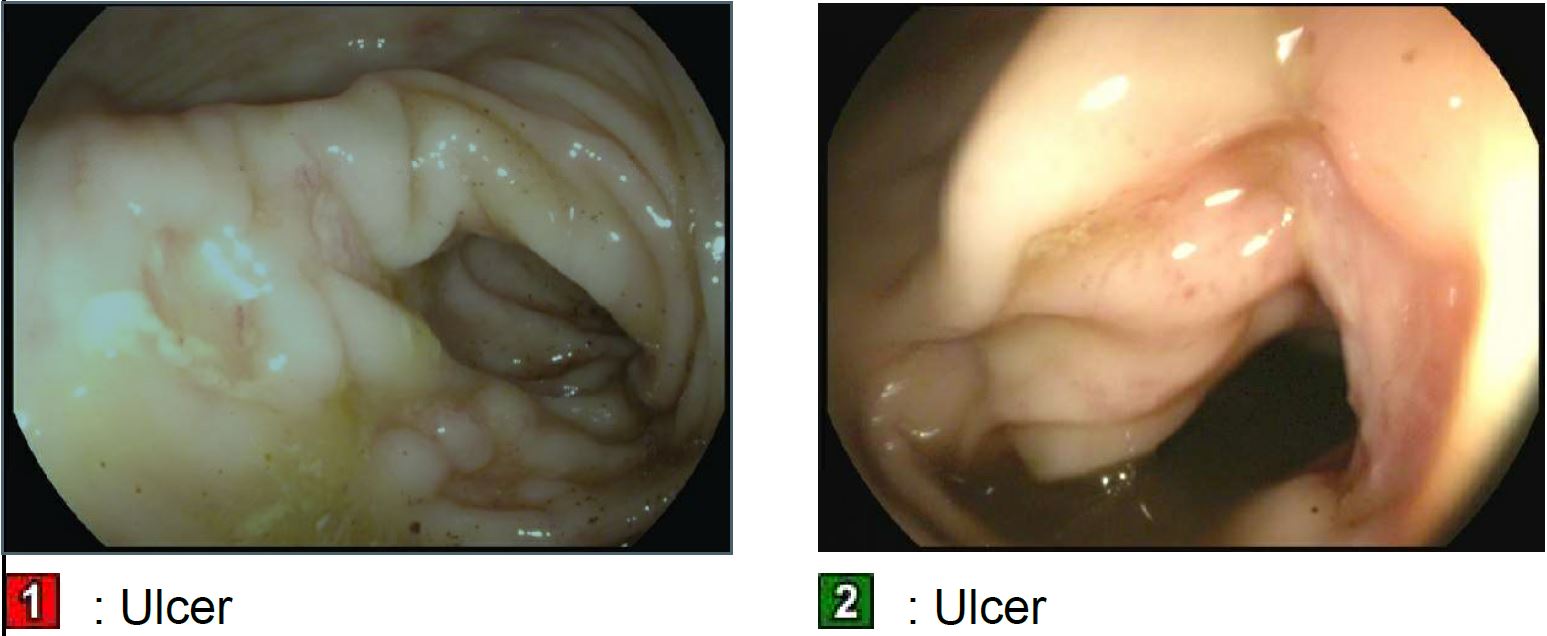
Case Presentation: A 58-year-old male with limited prior health care utilization with presumed longstanding untreated HTN, otherwise unknown medical history, presented to a rural hospital with lethargy, confusion, acute renal failure of unknown duration. His personal history is significant for being exposed to pigs and chicken. On exam, he had a left lower extremity wound with an irregular base and foul-smelling purulent drainage. After incision and drainage of the wound, he was started on Vancomycin and Piperacillin-tazobactam and received urgent hemodialysis. One of 2 sets of his initial blood cultures were positive for Salmonella spp. Drainage from his left leg wound grew Salmonella gallinarum.Due to profuse rectal bleeding, he was transferred to our facility due to lack of gastroenterology services. A colonoscopy was performed which showed multiple partially epithelialized ulcers in the transverse colon with a colonoscopic impression of ischemic colitis. Biopsy showed rare mild cryptitis and a crypt abscess suspicious for acute infectious etiology. No stool cultures were done to confirm whether this was related to Salmonellosis. Repeat blood cultures in our facility were sterile. Repeat wound cultures grew Salmonella enteritidis, group D. He was continued on Piperacillin-tazobactam. Due to poor wound healing, additional wound debridement was done. He had interval development of 2 additional abscesses on the medial aspect of his left leg and required additional surgery. Recurrence raised suspicion for an endovascular source, but echocardiogram and CT AAA were non-revealing. He was switched to Ceftazidime dosed with hemodialysis to complete 6-week antibiotic course and discharged for outpatient follow up.
Discussion: Only about 6% of non-typhoidal salmonella (NTS) infections cause bacteremia and this occurs most commonly in immunosuppressed populations.1 Our patient was at high risk of environmental exposure due to animal husbandry (pigs and chicken) and most recently his job involved removing dead chickens from coops. Salmonella gallinarum is known to cause “fowl typhoid” which could be his infectious source. From history, an exact temporal relationship could not be made in this case for gastroenteritis, bacteremia and the skin abscesses.In our case review, we have identified 2 prior case reports of a patients with multiple leg abscesses from NTS, which were S. enteritidis and S. hiedelberg.2,3 NTS infections rarely involves the skin and soft tissue. They usually occur among immunosuppressed and diabetic patients.2,4 There are rare occurrences of skin abscess as sole clinical manifestation.4 Commonly salmonella abscesses occur in the setting of bacteremia.4 For uncomplicated NTS gastroenteritis current guidelines do not recommend antimicrobial treatment. But for systemic illness antibiotic use can be warranted. If susceptible, treatment with an agent such as ceftriaxone, ciprofloxacin, TMP-SMX, or amoxicillin is recommended. CDC has reported emerging antibiotic resistance among Salmonella spp.5
Conclusions: – Our case adds to evidence that NTS rarely manifest as skin abscesses – NTS should be included in the differential especially in cases with high-risk environmental exposures, compromised immunity and recent or concomitant gastroenteritis.- NTS abscess can rarely occur as primary infection. – Once identified, treatment with an agent such as ceftriaxone, ciprofloxacin, TMP-SMX, or amoxicillin is recommended