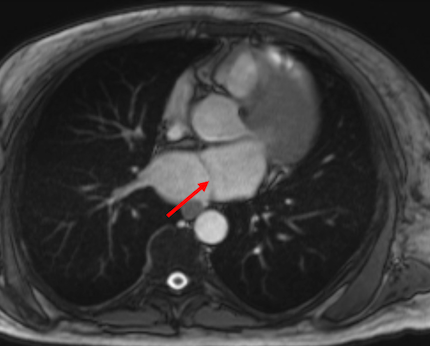
Case Presentation: A 47-year-old male with a history of heart failure with reduced ejection fraction, hypertension, and type 2 diabetes mellitus presented with acute, left-sided weakness. On arrival, his blood pressure was markedly elevated at 206/110 mmHg, and capillary blood glucose exceeded 500 mg/dL. EKG demonstrated atrial fibrillation (AF). Brain MRI confirmed multifocal acute infarcts, consistent with an embolic pattern. Transthoracic echocardiogram detected a severely dilated left atrium with a fibromuscular ridge; subsequent cardiac MRI confirmed a fenestrated membrane dividing the left atrium, consistent with a diagnosis of Cor Triatriatum Sinister (CTS), as well as asymmetric severe septal hypertrophy with late gadolinium enhancement raising concern for hypertrophic cardiomyopathy (HCM). The patient’s weakness improved, and he was started on apixaban 5 mg twice daily for embolic stroke prevention. He opted for a wearable cardioverter-defibrillator rather than pursuing inpatient ICD placement or catheter ablation. He was discharged in stable condition with general cardiology, electrophysiology, and adult congenital heart disease follow-up.
Discussion: CTS is a rare congenital cardiac anomaly, accounting for up to 0.4% of all congenital heart defects. It is characterized by a fibromuscular membrane that bisects the left atrium, potentially obstructing pulmonary venous return and leading to left atrial enlargement and arrhythmias, most notably AF. Although typically diagnosed in childhood, CTS may remain clinically silent until adulthood, with initial symptoms often stemming from complications such as heart failure, arrhythmia, or stroke. This unique case describes a patient with CTS and suspected HCM who presented with a cardioembolic stroke in the setting of AF. The presence of these two structural abnormalities may synergistically amplify the risk of arrhythmia and embolic complications. Early recognition of rare congenital anomalies such as CTS should prompt consideration of timely anticoagulation and coordinated, multidisciplinary care to reduce the risk of cerebrovascular events.
Conclusions: This case raises awareness of rare congenital anomalies like CTS which can lead to AF and embolic stroke, presentations commonly encountered by hospitalists. The co-occurrence with structural abnormalities such as HCM further highlights the need for timely, expert consultation to achieve coordinated care and prevent recurrence.