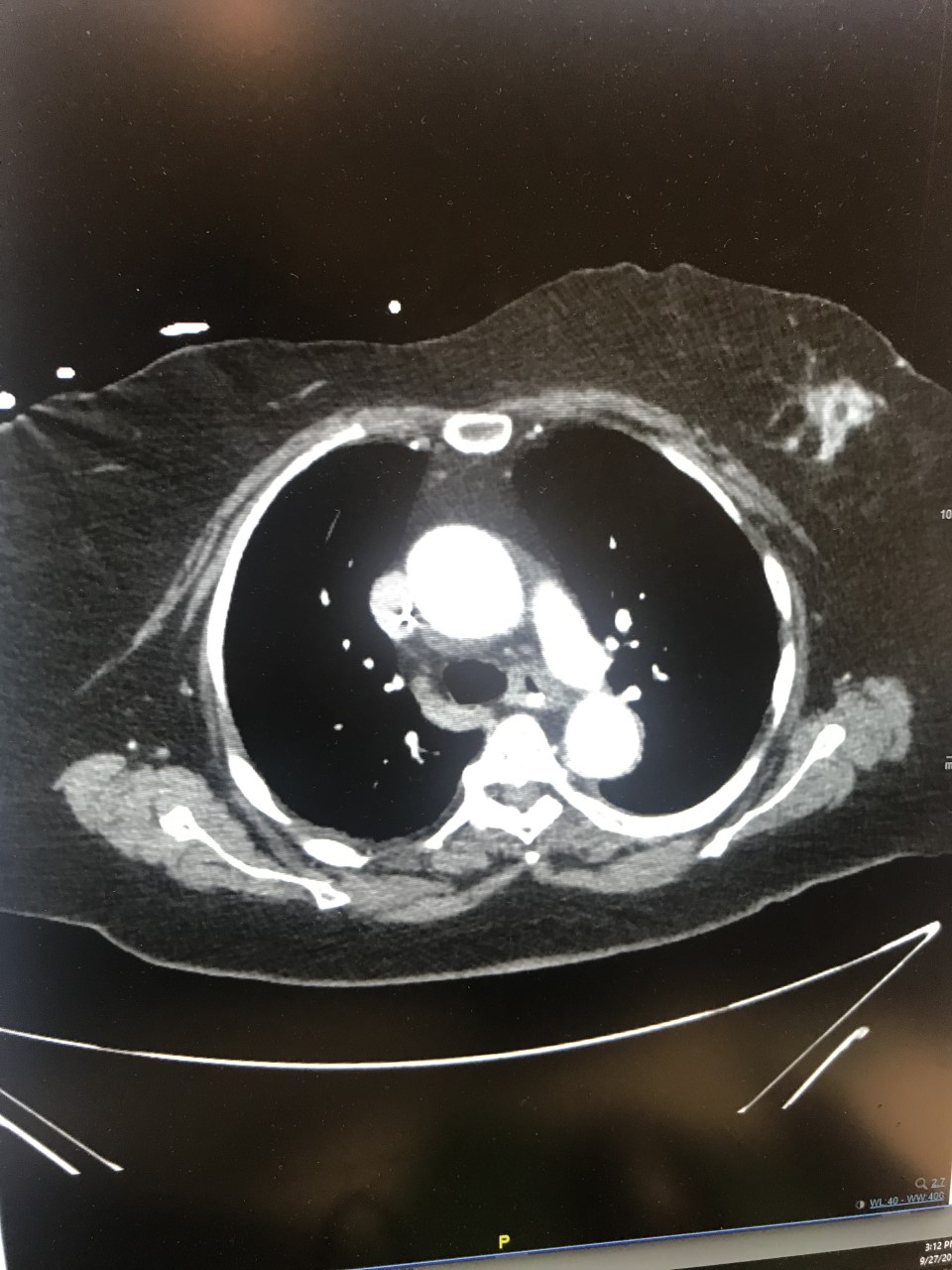
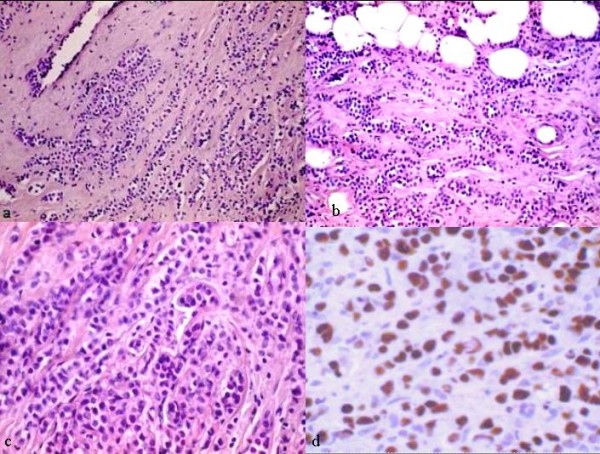
Case Presentation: A seventy nine year-old female with a past medical history of hypertension presents to the Emergency Department with abdominal pain. She reports a decrease in appetite for a few months as well as increasing abdominal discomfort. Her abdominal pain had started three days before and she describes it as “being punched in the gut.” A CT scan of her abdomen and pelvis reveals a hypoattenuating appearance in the pancreatic head concerning for a mass as well as severe distention of the gallbladder and diffuse biliary ductal dilation. Severe gastric distention concerning for complete gastric outlet obstruction was also noted. A nasogastric tube is placed and surgical oncology is consulted, they recommend that gastroenterology be consulted to perform an ERCP/EUS and FNA of the mass. Tumor markers CA 19-9, CEA and CA 125 are obtained and are all within normal limits. Gastroenterology performs the biopsy and places a duodenal stent for symptomatic relief. This biopsy reveals adenocarcinoma with signet ring cells, which are consistent with diffuse type adenocarcinoma. We obtain a CT chest to stage the suspected gastric adenocarcinoma. This scan reveals a 3x2cm spiculated mass in the left breast. An ultrasound guided biopsy is obtained and the initial pathology report reveals a poorly differentiated carcinoma with occasional signet ring cells, thought to be a metastasis from her primary gastric cancer. As the patient’s symptoms are relieved, she is discharged from the hospital with plans for her case to be discussed in Tumor Board conference. Meanwhile, additional immunostaining is done of the breast biopsy that reveals it is ER/PR +. Similar stains are done on the duodenal biopsy sample with similar results. This lead to the conclusion that the primary cancer is an invasive mammary lobular carcinoma that had metastasized to the duodenum, causing the gastric outlet obstruction. The patient is initially started on armidex but she and her family decide to pursue hospice.
Discussion: Breast cancer is the most common cancer among females, contributing 25% of total new cancer diagnoses in women (1). The usual presentation of a primary breast lesion starts as local or regional symptoms. If the breast cancer is metastatic, the presentation behaves according to the site of the metastasis. The most common sites of metastases are lung, liver, and bone. GI metastases only occur in 4%-18% of women (1), with invasive lobular carcinoma most likely to metastasize to the GI tract (2). When breast carcinoma metastasizes to the GI tract, it is important to differentiate it from a primary gastric carcinoma, as the treatment plans for these two malignancies are different (3). The signet ring cell feature is characteristic of not only gastric but also of other GI adenocarcinomas, and this feature can add to the diagnostic dilemma in such cases (4). In our case, gastric outlet obstruction was the first manifestation of metastatic breast cancer in a patient who had no breast symptoms. As such, tissue samples and histopathology was essential to our diagnosis of metastatic breast cancer
Conclusions: In conclusion, tissue samples can be the key pieces to diagnosing cancer. In our patient in particular, it was the duodenal tissue sample and immunostaining that differentiated the presenting mass as a metastasis rather than a primary GI malignancy, despite its uncommon location. This then allowed the patient to be started on the correct treatment plan. This case serves as a reminder of the importance of having a broad differential when initially evaluating patients.