Background: Medicare observation stays are increasing nationally. Beneficiaries frequently hospitalized under observation, as well as those needing post-acute care skilled nursing facility coverage, may face increased financial burdens from these services. Patients living in the most disadvantaged neighborhoods have increased risk of inpatient 30-day re-admissions. It is not known whether neighborhood socioeconomic disadvantage increases 30-day re-observation risk.
Methods: This retrospective study of a 2014 20% Medicare fee-for-service beneficiary cohort included 319,980 observation stays among 273,308 beneficiaries. We evaluated risk of a 30-day re-observation following an index observation stay for those living in the most disadvantaged compared to the least disadvantaged neighborhoods.
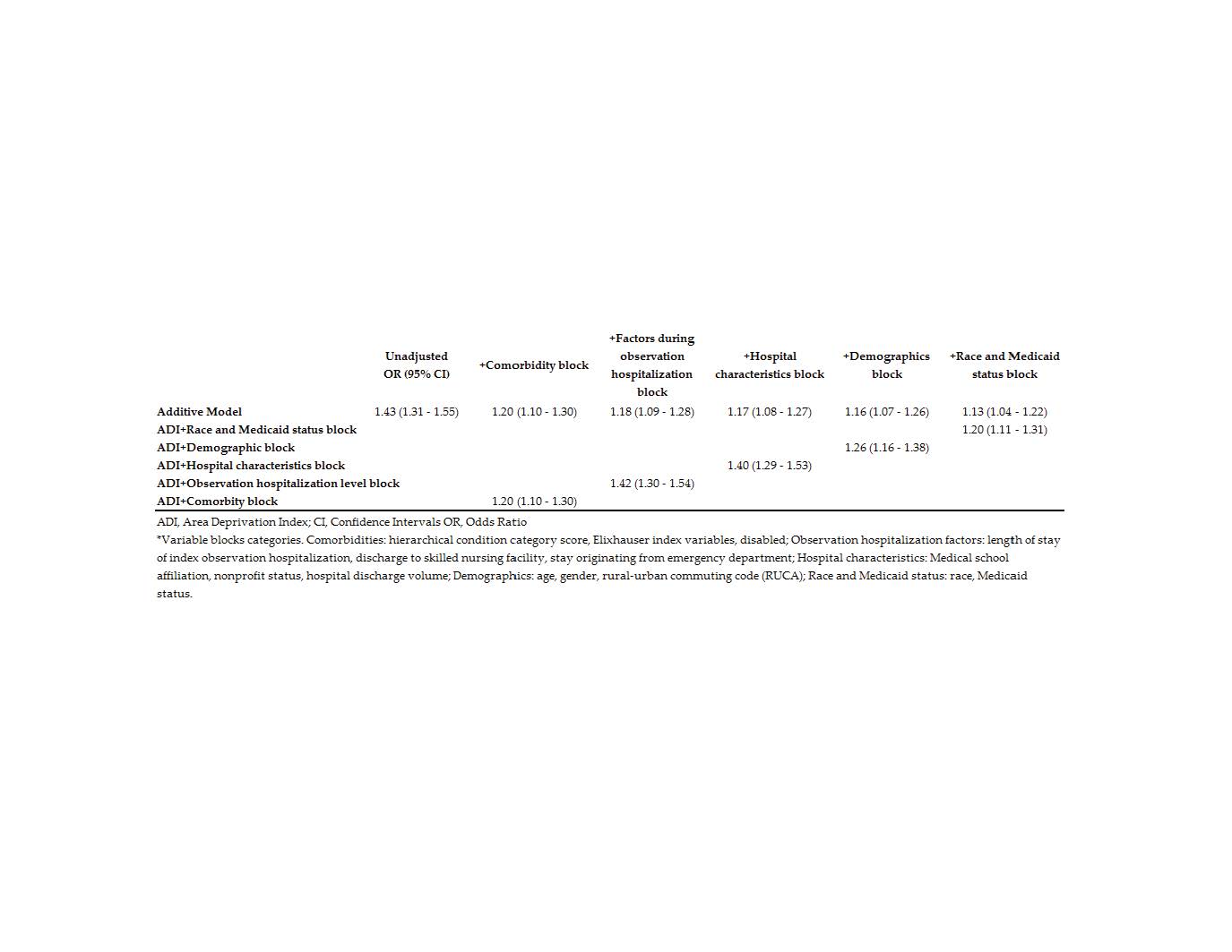
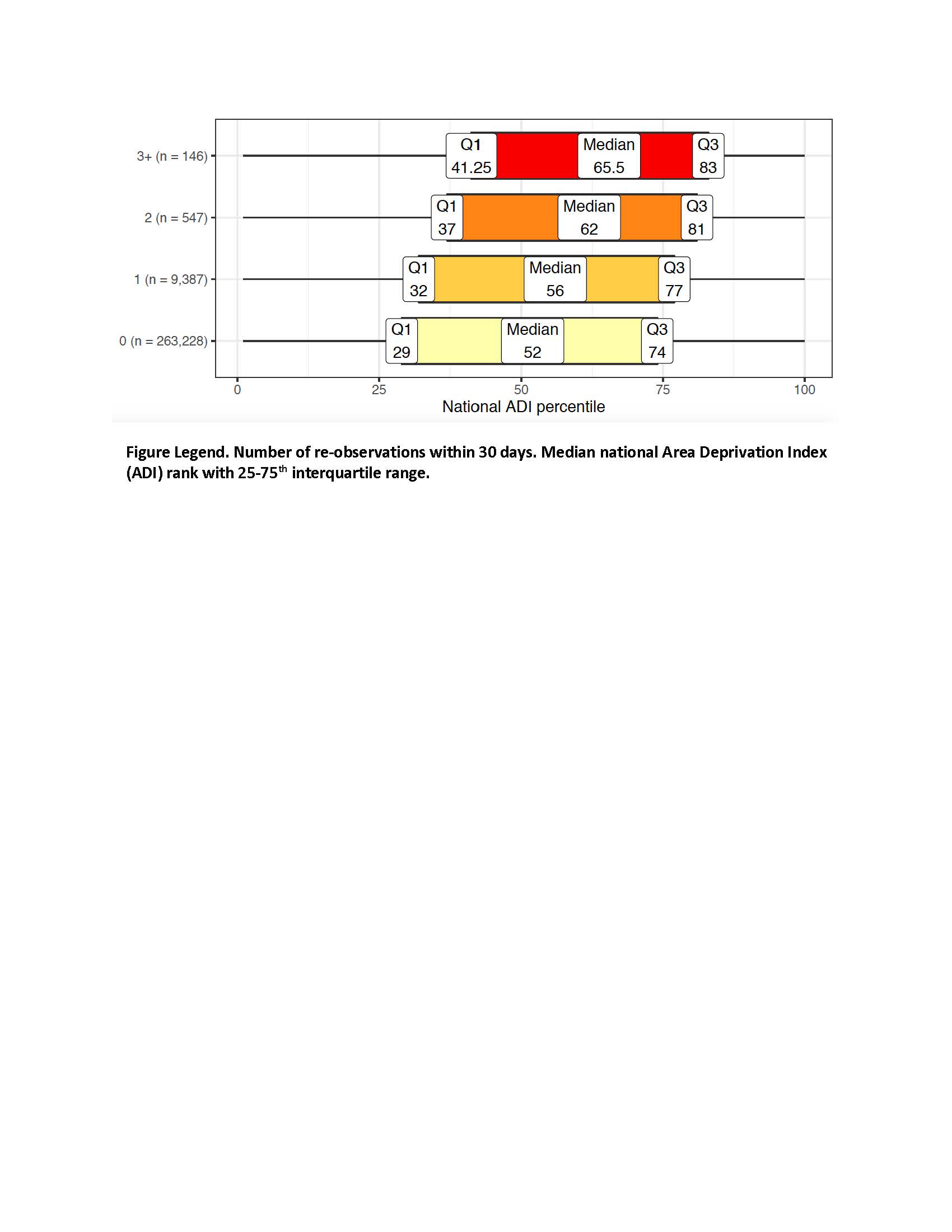
Results: Patients in the most disadvantaged neighborhoods had higher 30-day re-observation rate (6.8%) compared to least disadvantaged neighborhoods (4.9%), a 43% increased risk (unadjusted OR 1.43 [1.31-1.55]). After adjustment, this increased risk remained (1.13 [1.04-1.22]) (Table 1). Discharge to skilled nursing facility reduced 30-day re-observation risk (OR=0.63), while index observation length of stay of four or more days conferred increased risk (OR=1.29); those living in disadvantaged neighborhoods were less likely to discharge to skilled nursing facilities and more likely to have long index stays. Beneficiaries with more than one 30-day re-observation (‘chronic re-observation’) had progressively greater disadvantage by number of stays (adjusted IRR=1.08 [1.02-1.14]) (Figure 1). Observation prevalence varied nationally.
Conclusions: Thirty-day re-observation, and especially ‘chronic re-observation’, is highly associated with socioeconomic neighborhood disadvantage, even after accounting for factors such as race, disability, and Medicaid eligibility. Beneficiaries least able to pay are potentially most vulnerable to high costs from serial re-observations, which may discourage patients from seeking necessary care.