Case Presentation: A 38-year-old African American female with recurrent oral-genital ulceration deemed of unclear etiology presented to the hospital with acute abdominal pain. Abdominal imaging demonstrated multiple intraabdominal venous thromboses, including hepatic venous involvement and hepatic venous outflow obstruction consistent with Budd-Chiari Syndrome (BCS). Extensive hypercoagulable workup was unremarkable. She was started on anticoagulation but was not diagnosed with BD then. The clinical course was complicated by cirrhosis followed by a late presentation with subacute neurological symptoms that led to the diagnosis of BD after brain biopsy findings were consistent with NeuroBehcets. Pulse dose steroids were given, and she was placed on Azathioprine and Adalimumab with significant improvement of symptoms.
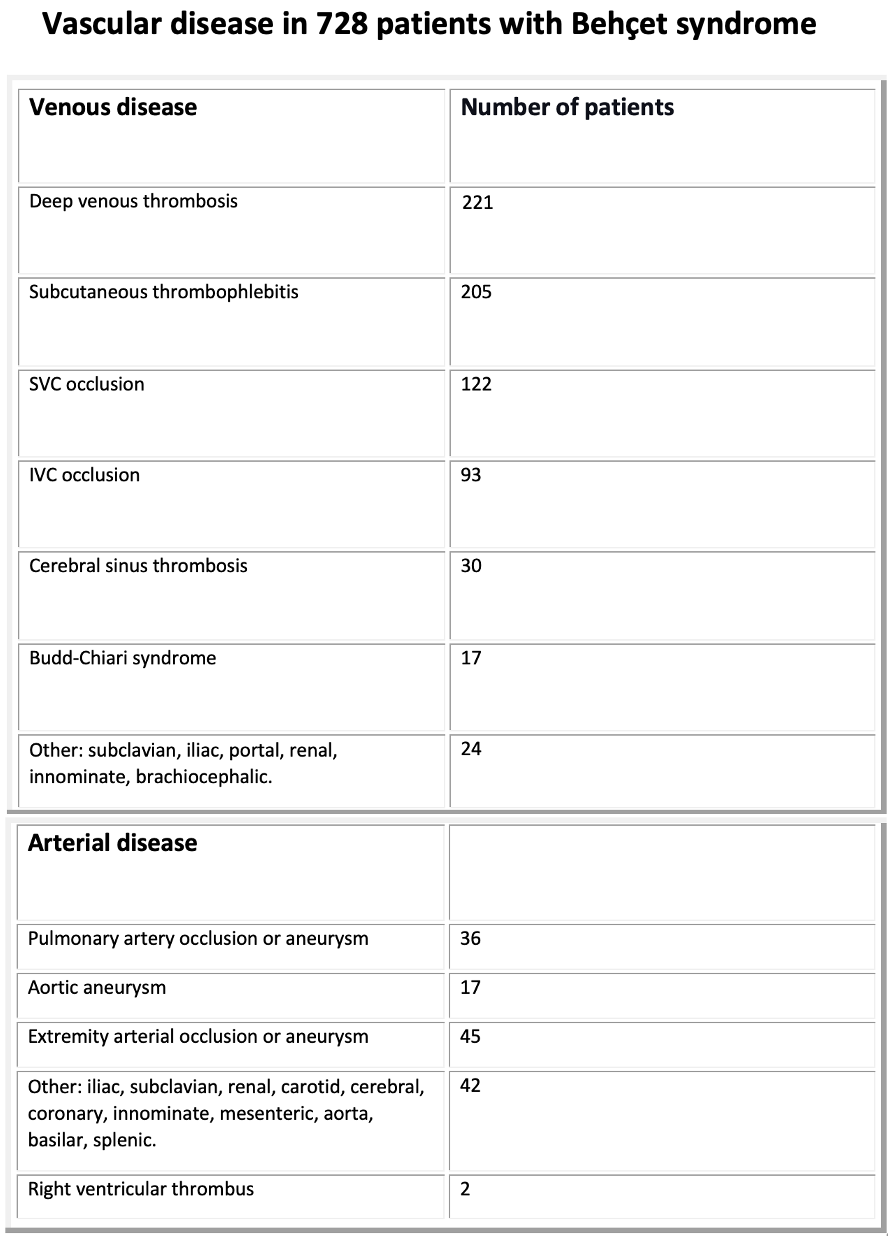
Discussion: Behçet disease (BD) is a chronic multisystem inflammatory disorder characterized by mucocutaneous ulcerations and multisystem involvement. It was first described by Hippocrates in the 5th century BC. Then it was brought to the medical community’s attention in the early 1930s by Hulusi Behçet, a Turkish professor of dermatology, after noticing recurrent presentation with a triad of oral aphthous ulcers, genital ulcers, and ocular disease. Most clinical manifestations of Behçet syndrome are vasculitic, with venous thrombosis being more frequent than arterial involvement. The underlying etiology remains unclear. It is thought to result from an aberrant immune activity triggered by environmental factors in genetically predisposed individuals. Nowadays, BD is prevalent along the silk road, an ancient trade route linking the Western world with the Middle East and Asia. It is most common in Turkey at 80 to 370 cases per 100,000. Estimates of prevalence in the United States and Europe have ranged from 0.12 to 7.5 per 100,000. It typically affects young adults 20 to 40 years of age. Most cases of Behçet syndrome are sporadic, but familial clustering has been reported. Vascular involvement is seen in up to 30 percent of patients with BD. It is one of the principal causes of morbidity and mortality. The most common form of venous involvement is lower extremities deep venous thrombosis followed by subcutaneous thrombophlebitis. Arterial disease is typically manifested as aneurysms; arterial occlusions are seldom seen. The approach to preventing venous thrombotic events in Behçet syndrome is the control of systemic inflammation rather than the institution of primary anticoagulation. BCS is defined as hepatic venous outflow tract obstruction. It is a rare but serious complication of BD, with a reported prevalence of 3.2 percent. Endothelial dysfunction resulting from vascular inflammation is considered an essential factor of thrombosis in BD. Treatment for BCS in patients with BD should include glucocorticoids combined with another immunosuppressive agent and lifelong anticoagulation. Based on a previous study, patients treated with Adalimumab achieved faster steroid tapers and a more effective and rapid resolution of venous thrombosis than other immunosuppressive therapies
Conclusions: The presence of BCS should raise clinical suspicion for BD, particularly in patients with recurrent oro-genital ulcerations and ocular manifestations. That association was missed in our patient. Early recognition and immunotherapy initiation can alter the disease course in BD and prevent debilitating vascular complications such as BCS.