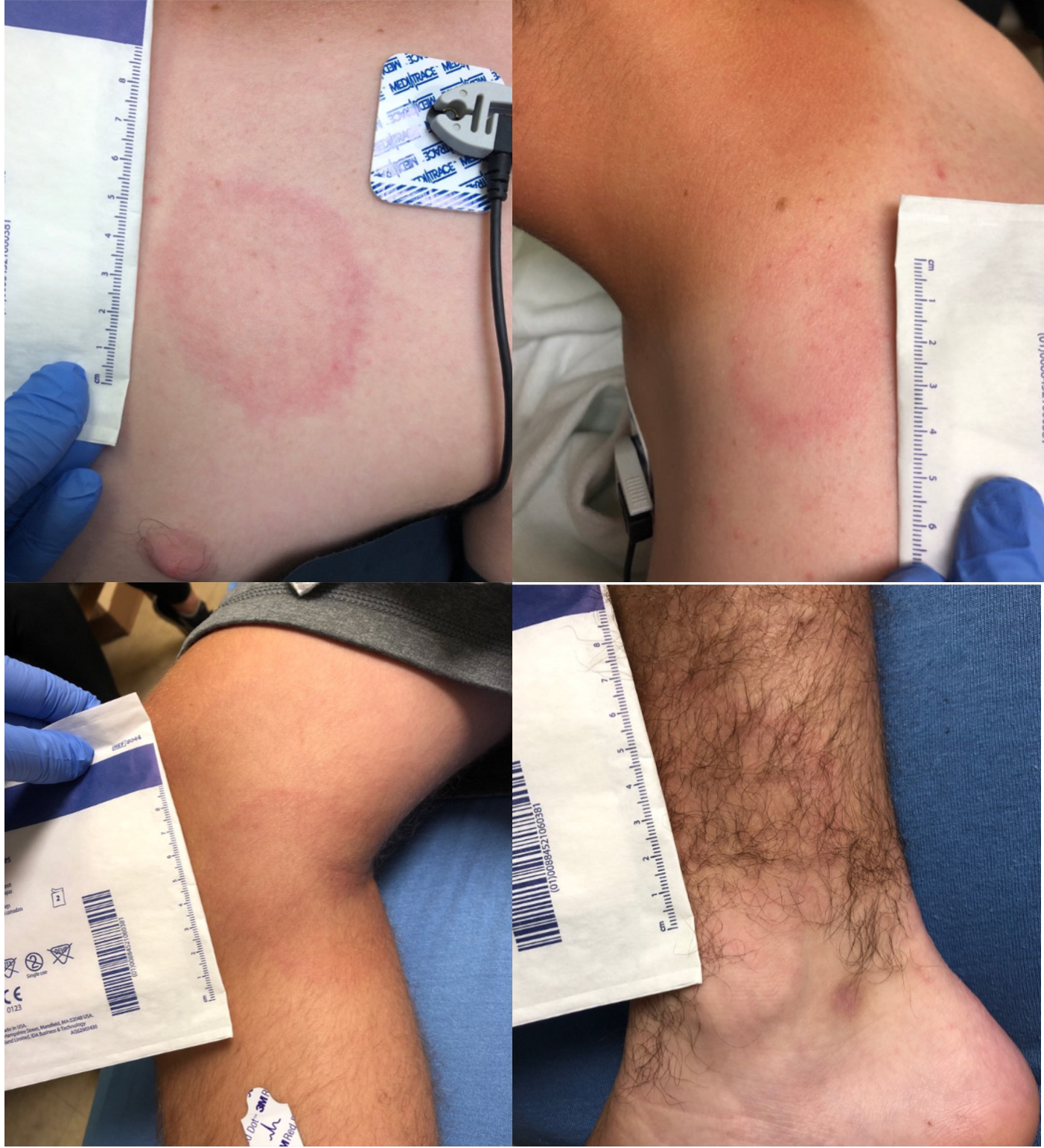
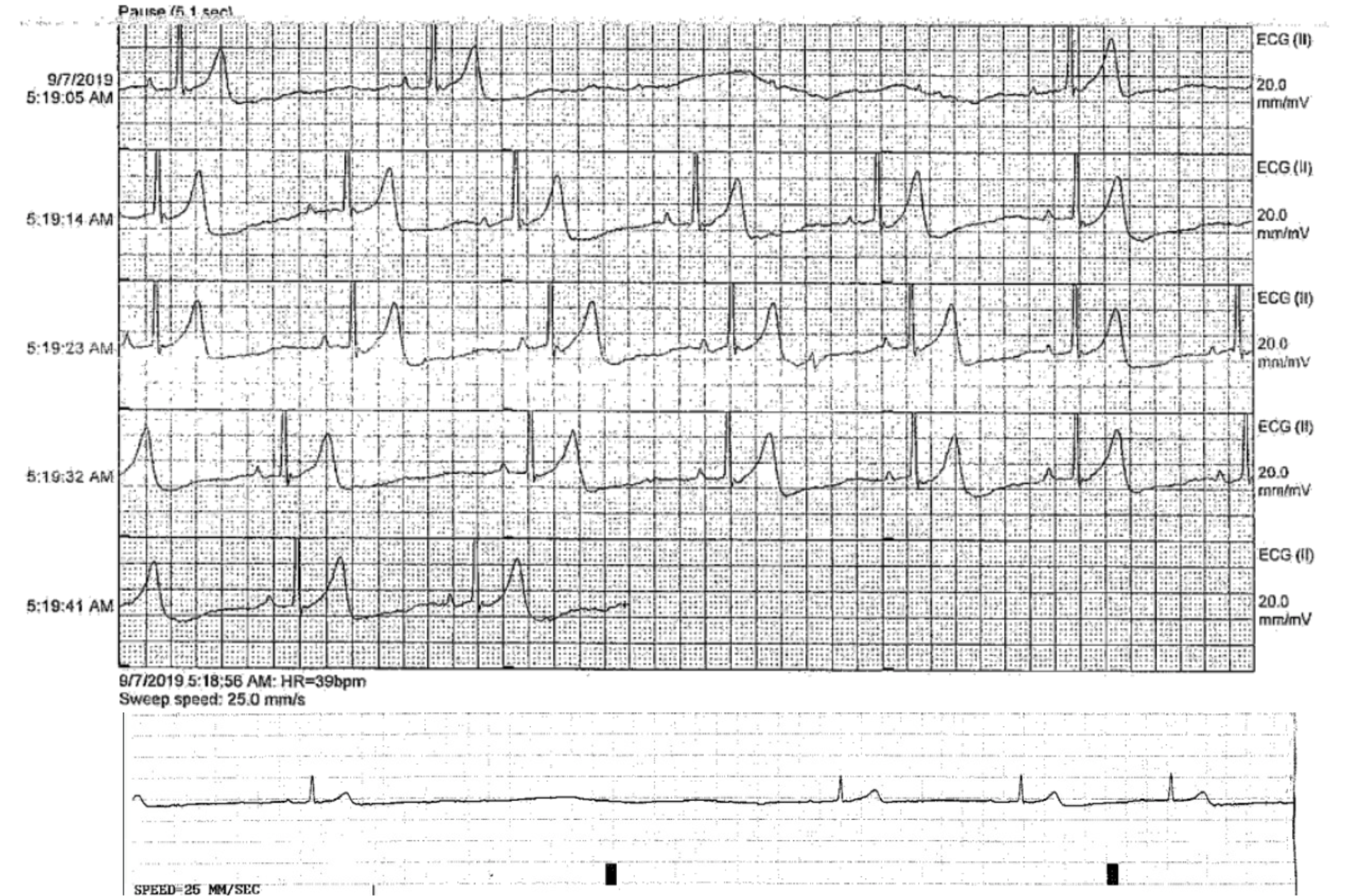
Case Presentation: A 16 y/o male presented with an acute onset of palpitations, generalized chest pain, and rash (Figure 1). In light of recent camping exposure and targetoid lesions compatible with erythema chronicum migrans (ECM), Lyme disease was suspected. An EKG demonstrated 1st degree AV block with a PR interval of 384 msec. Echocardiogram and troponin were reassuring against pan-carditis. Lyme IgM and western blot returned positive. The patient was admitted for telemetry and IV ceftriaxone. There was complete resolution of erythema migrans within two days of treatment. During the first week of hospitalization, he was noted to have sinus pauses and possible 2:1 heart block on telemetry (Figure 2). Given his clinical stability and a reassuring stress test, expectant management was observed. The patient was treated with IV ceftriaxone for 10 days with continuous cardiac monitoring until sustained stabilization of the PR interval at <200 msec was demonstrated. His PR interval normalized to <176 msec after 10 days of parenteral treatment. He was transitioned to oral doxycycline and discharged home to complete a 28-day course of antibiotics. Extended ambulatory cardiac monitoring confirmed the resolution of the previous observed EKG changes.
Discussion: Lyme disease (LD) is the most common tick-borne illness in North America. Climate change has resulted in an increased prevalence of LD, even in hyper-endemic regions of the upper Midwestern US. Although an unusual manifestation of LD, hospitalists should be aware of the risk of carditis as a potential complication.Lyme carditis results from direct invasion of the spirochete into the myocardium with subsequent immune response causing inflammation. In contrast to the neutrophilic response exhibited in Lyme arthritis, lymphocytes and macrophages are primarily involved in Lyme carditis. AV nodal block is the most common manifestation of Lyme carditis. It is not entirely clear why the AV node is most commonly affected, but it is postulated that its anatomic location, histology and metabolic mechanisms may play a role. Autoimmune response may contribute to injury as well, with antibodies produced during initial exposure reacting to self-components.Current guidelines recommend that any patient with cardiac symptoms such as syncope, chest pain, or EKG changes be admitted for telemetry. The risk of untreated 1st degree AV block is progression to 3rd degree heart block, which can be fatal. Guidelines suggest management with IV ceftriaxone (first-line) for 10-14 days followed by oral antibiotics to complete a total antibiotic course of 14-21 days. In Lyme-endemic areas or in the setting of ECM with a compatible clinical presentation, empiric antibiotic treatment should be administered while definitive diagnostic studies are pending. Overall, Lyme carditis has a favorable prognosis. Temporary pacemaker placement is recommended if the PR interval fails to normalize within 14 days post-admission.
Conclusions: In patients who present with signs and symptoms concerning for LD with cardiac symptoms, it is vital to consider EKG and hospitalization for continuous cardiac monitoring and intravenous antibiotics. With the rising incidence of Lyme disease in the Midwest, providers must maintain a high level of suspicion in order to promptly diagnose and treat Lyme carditis, as well as prevent unnecessary pacemaker placement in the pediatric population.