Background: Hospitals emphasize early discharge to improve throughput. Interdisciplinary team members often report feeling rushed in the 24 hours before discharge, which may increase the likelihood of discharge errors and burnout for the team.
Purpose: To identify obstacles preventing timely completion of discharge activities, improve reliability of the discharge process, improve staff experience, and decrease avoidable days.
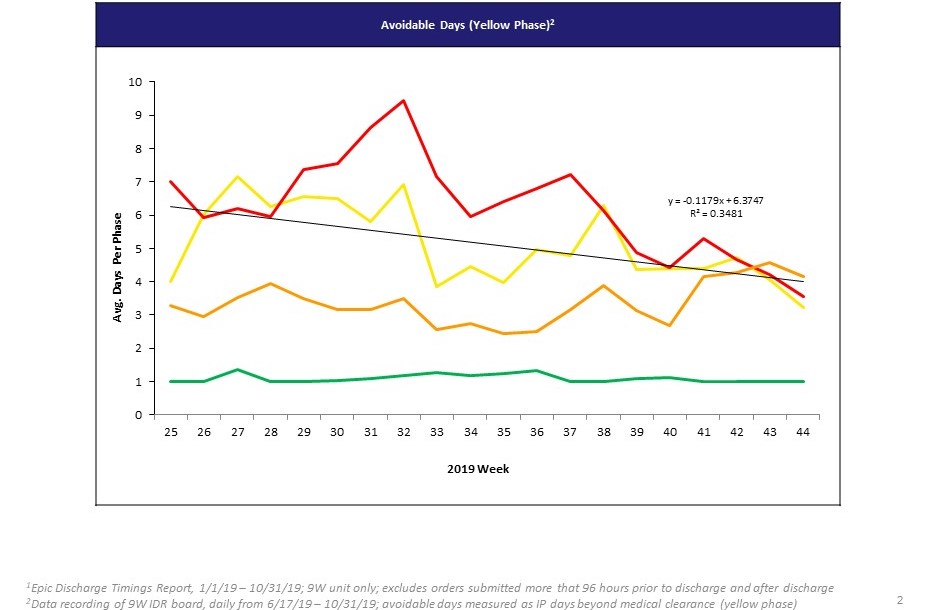
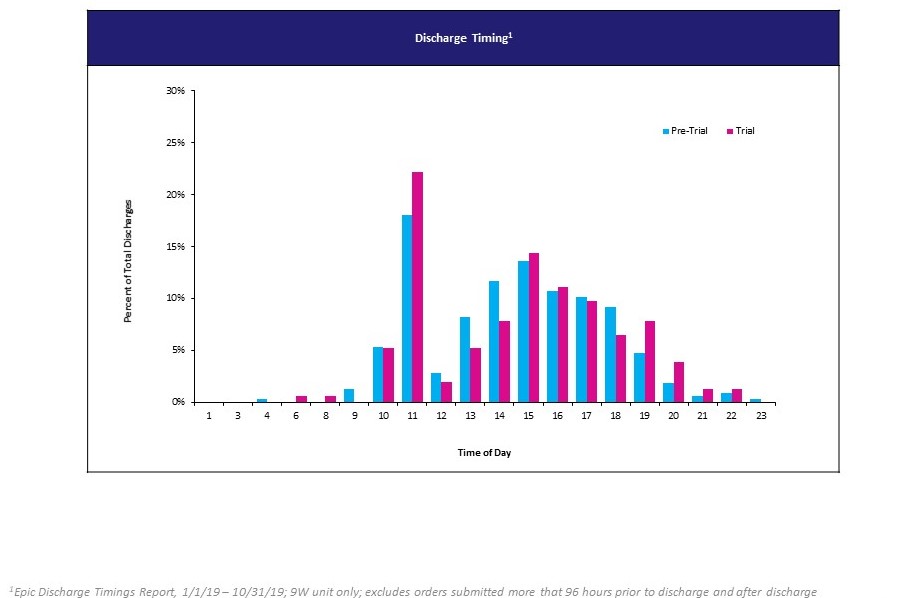
Description: This project was conducted on one 25-bed medicine unit at an urban tertiary-care 1,100-bed academic teaching hospital. Physician teams were not geographically organized. Unit-based staff included case managers (CM), social workers (SW), nurses (RN), pharmacists, and physical therapists. The team of interdisciplinary staff used continuous improvement tools and activities to understand current state discharge processes, including cross-functional process mapping, information flow mapping, observations, interdisciplinary work groups and data collection. They identified that there was no standard method to track patient progression towards discharge, resulting in functional silos and redundant communication and work by the interdisciplinary team.A pilot was designed to test a shared visual management system during daily interdisciplinary rounds (IDR) to improve operational stability by creating a shared mental model of patient status, which would assist staff in prioritizing work. Each patient’s status was categorized across four phases: Red (acutely ill), Orange (forecasting medical readiness in the next 24-48 hours), Yellow (medically ready but pending needs, such as home services or insurance authorization), and Green (ready for discharge). The Yellow phase was used as a proxy for avoidable days. Each day, the physician presented the patient status at IDR. The unit team reached consensus on the phase designation, and the unit nurse manager recorded the phase on the visual management whiteboard. Iterations included adding a column to the whiteboard for remaining barriers to discharge to allow for closed loop communication. 256 patients were tracked, of whom 140 were discharged from the unit. Preliminary measures to assess impact included lead time (time before discharge) for implement discharge plan order (IDP), length of stay (LOS), avoidable days, and qualitative impact on process predictability. We did not find a significant difference between pre- and post-intervention periods for IDP lead time or LOS. A linear regression trend showed a decrease in Yellow days (R^2=0.3, Figure 1). Discharges before noon increased by 3% (Figure 2). A qualitative survey was distributed to 26 RNs (100% completed) and showed improvements in predictability, clarity about discharge timing, and ability to prioritize daily work (96%, 100% and 100%, respectively). During informal interviews, nurse managers reporting using the board for general unit planning, even outside of IDR. CM reported increased confidence in prompting teams for discharge tasks.
Conclusions: The use of a jointly created interdisciplinary visual management system on a non-geographic unit to identify patient status led to a perceived improvement in discharge planning and higher predictability of workflow, with trends suggesting an improvement in hospital level metrics. A sustainability plan was developed and the visual manager has transitioned to standard practice. The positive nature of included metrics indicates progress towards consistency and standardization in discharge processes.