Background: Patient experience (PEX) is associated with higher levels of adherence to recommended prevention and treatment processes, better clinical outcomes, improved patient safety within hospitals, and decreased inappropriate health care utilization. (1,2,3) Furthermore, overall patient satisfaction is associated with lower 30-day risk standardized hospital readmission rates after adjusting for clinical quality. (4) Our hospital medicine team sought to improve PEX by optimizing the environment of care and transforming the service’s culture.
Methods: In 2018, we embarked on a mission to improve patient experience on our hospital medicine (HM) service providing care to a vulnerable patient population at a 900-bed academic, urban safety net hospital in the southwestern United States. We developed a PEX leadership infrastructure including a PEX committee and a medical directorship for HM PEX. The PEX committee and leadership shared a variety of communication tips including saying your patient’s name, sitting, calling patients post discharge, and asking permission before examination to give HM faculty the tools to improve PEX. Our team also disseminated specific positive feedback in a multimodal communication strategy. HM leadership also decreased the daily census per rounder to increase time available for bedside visits and family meetings. Additionally, we incorporated PEX into the onboarding program, annual evaluations, incentive metrics and performance dashboard. To assess the effectiveness of our PEX interventions, we performed a retrospective cohort study on patients admitted to the HM service from 2016 through 2022. Means were compared between pre and post groups as well as physician groups (HM and All Physicians) using a student’s t-test. Differences in Differences (DID) analysis was performed with a General Linear Model (GLM) with Pre/Post and Physician group in the model as main effects. The interaction of these variables was evaluated. The significance level for all statistical tests was 0.05. SPSS (version 25) was used to perform statistical tests.
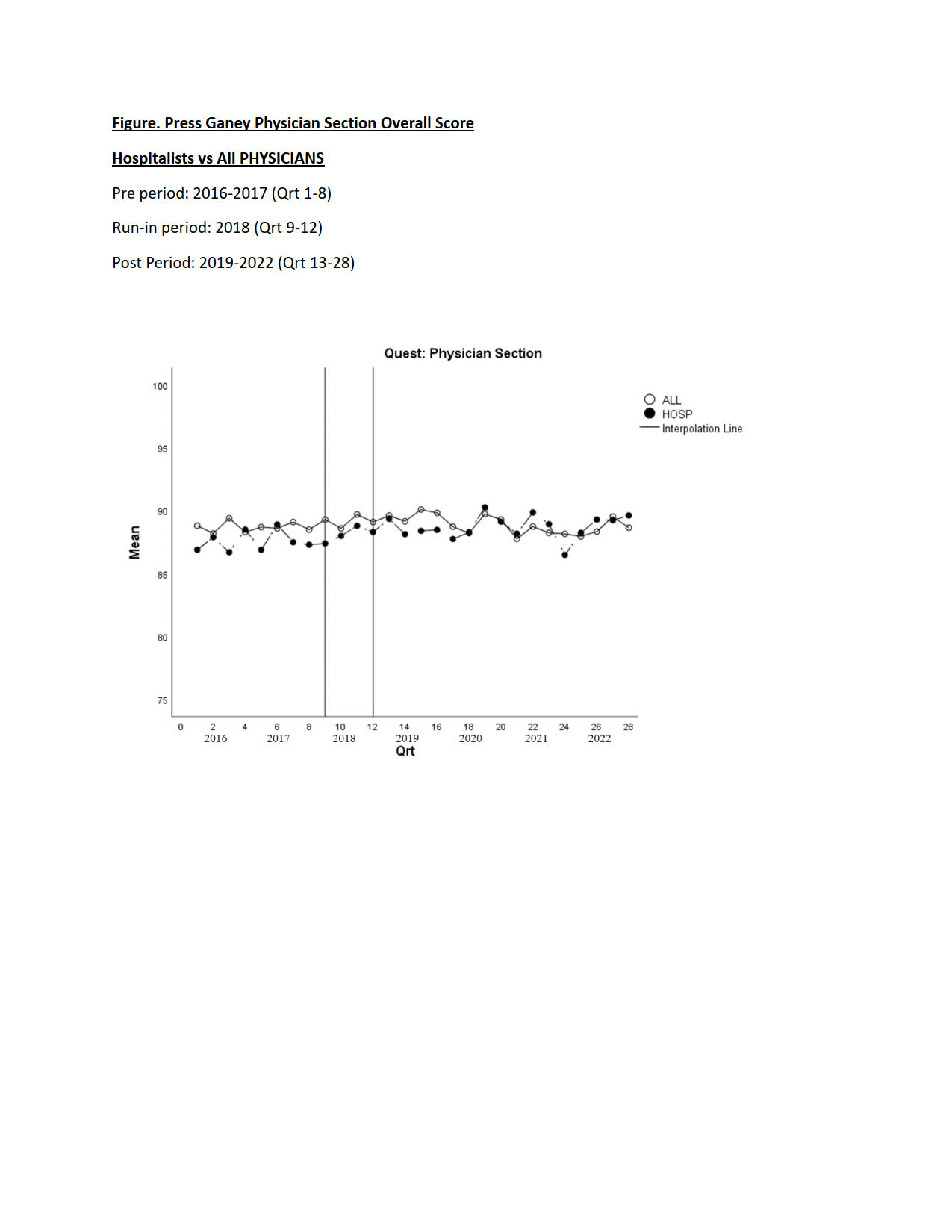
Results: Hospital Medicine physicians showed significant improvement in patient satisfaction scores for each physician-specific question in the Press Ganey survey over a six-year period, while the all-physician cohort did not show a significant improvement in scores in any of the domains assessed over the same time-period. The differences in differences analysis demonstrated that HM physicians experienced a much greater magnitude of improvement in each survey question when compared to all physicians (Table). The PEX dimension with the greatest difference in differences was “physician kept you informed” (DID = 1.5, p=0.006). The overall HM team PEX scores rose from the third quartile to the first quartile of academic medical centers. Hospital Medicine PEX trend as compared to All Physicians over the course of the study period is seen in the Figure.
Conclusions: Environmental shaping through formation of a PEX committee and medical directorship, sharing best practices, lowering census, and providing dashboard performance data in conjunction with cultural transformation through leadership messaging, positive reinforcement of success and financial incentives fostered the improvement of our patients’ experience. Our data suggests that both transactional and transformative change management levers may be applied to positively affect patient experience.