Background: Timely, effective follow-up after hospital discharge can improve the efficiency and outcomes of care by increasing hospital throughput and decreasing readmissions and other adverse events after discharge. The University of Chicago Medical Center (UCMC) has chronic bed shortages and a medically and socially complex patient population that makes optimal management of post-discharge care especially important. We established a post-discharge clinic (PDC) to address the needs of patients, hospitalists, and primary care physicians (PCPs) to improve ambulatory care access within 14 days post-discharge, improve quality of care and operational efficiency.
Purpose: Assess the PDC’s effectiveness on primary care access within 14 days post-discharge, adverse events identification and readmission
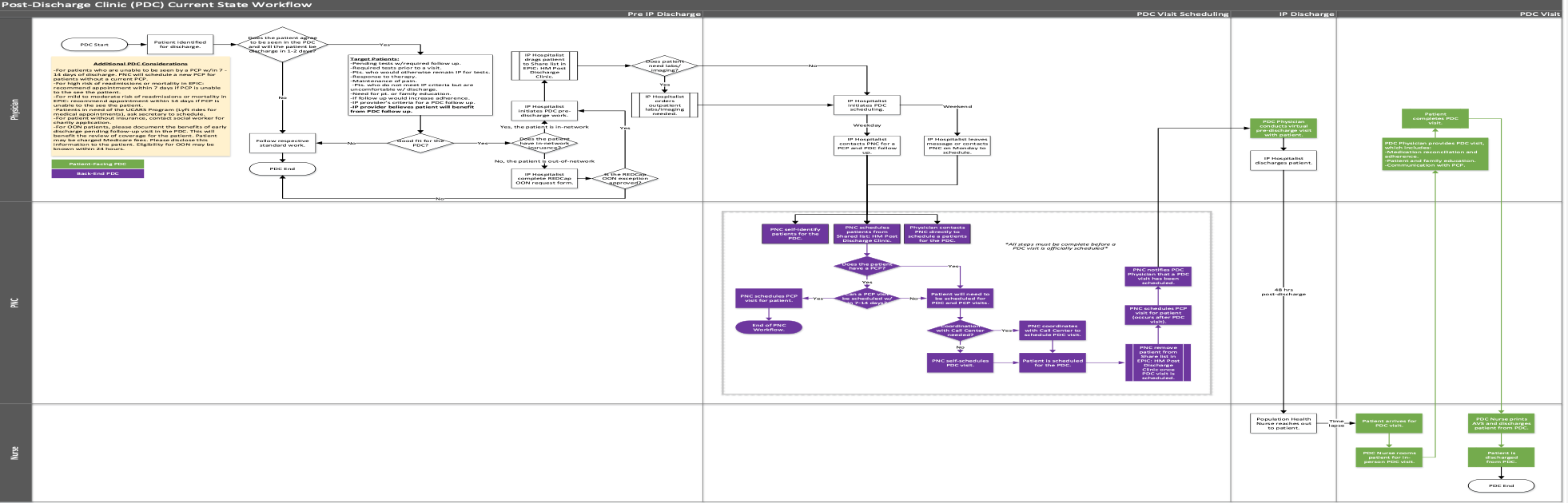
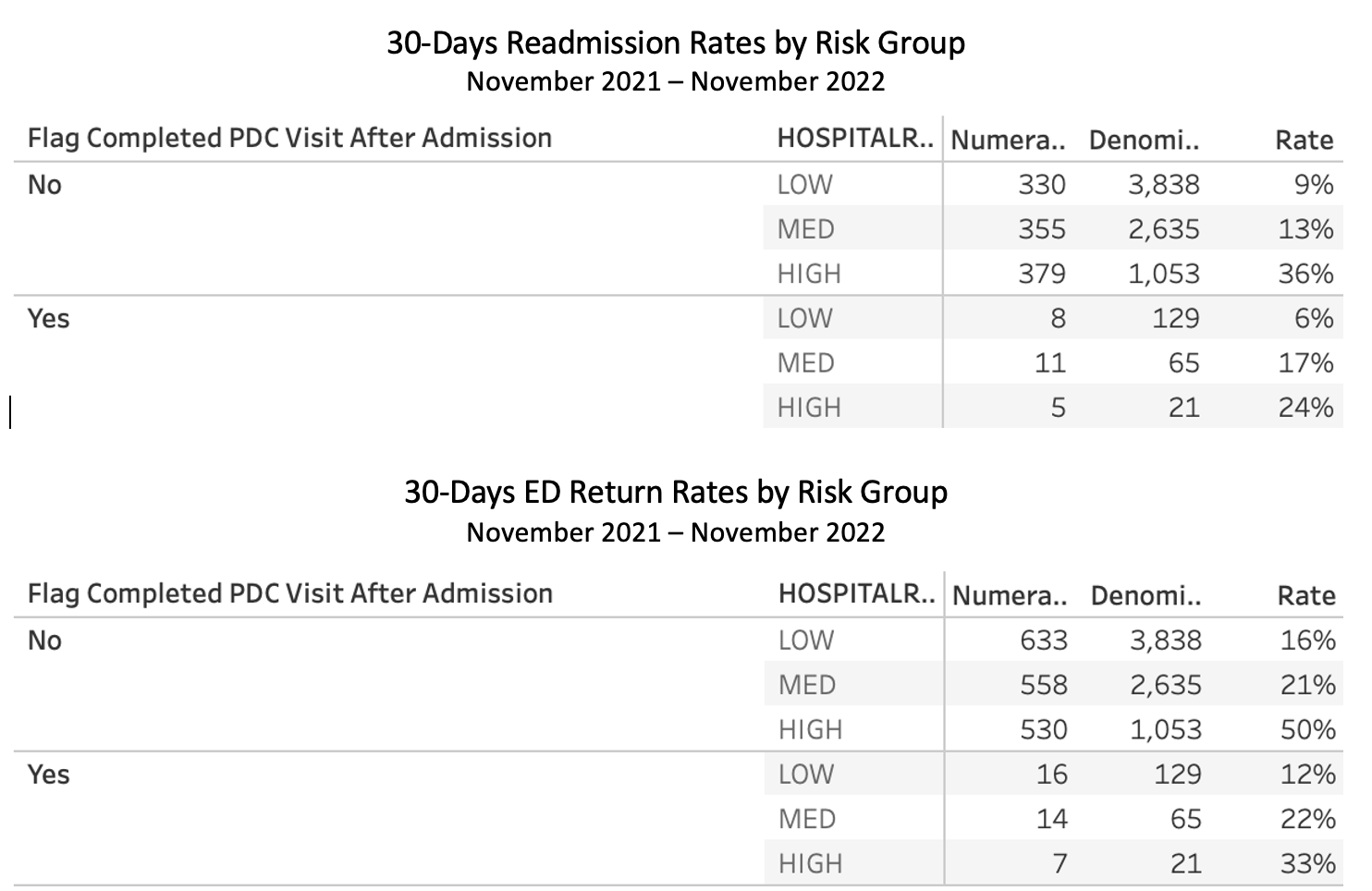
Description: The PDC created a multimodal care pathway to facilitate smooth transitions from inpatient to outpatient care. Three workflows were developed.1. Patient Identification: Patients were identified based on criteria that meet the needs of patients and the organization to decrease length of stay and readmissions.2. Scheduling: A novel self-scheduling system allowed Patient Navigation Coordinators (PNCs) to schedule patients directly in the PDC providers’ schedule.A shared folder in EPIC was created in which inpatient providers could enter the patient information for the PNCs to schedule.3. Clinic Flow: We mapped a lean workflow. PDC visits were offered both in-person and virtually via MyChart and Doximity. The PDC partnered with UCM finance to determine an out-of-network workflow. The PDC partnered with the Population Health team for 48-hour RN post-discharge phone visits. The PDC was able to participate in the Transitional Care Management (TCM) Program.Patient Access: The time between discharge and being seen in the PDC is less than 14 days post-discharge. For discharged patients establishing new primary care at UCMC, the average lead time is 61 days.Identification of Adverse Events and Readmissions: We were able to identify and intervene on adverse events and measured the outcomes on 30-days readmission and Emergency Department (ED) return rates by risk groups. Readmission and ED return rates were compared for patients attending the PDC and patients not attending the PDC by the Data Analytics Department. Patients seen at the PDC have significantly less 30-days readmission and ED return rates as compared to patients not seen at the PDC.
Conclusions: The PDC seeks to improves UCM care access, quality and outcomes by providing transitional care access to patients discharging from the hospital within 30 days of hospitalization. Evidence show improved access to post-discharge care and reductions in readmissions and ED visits.