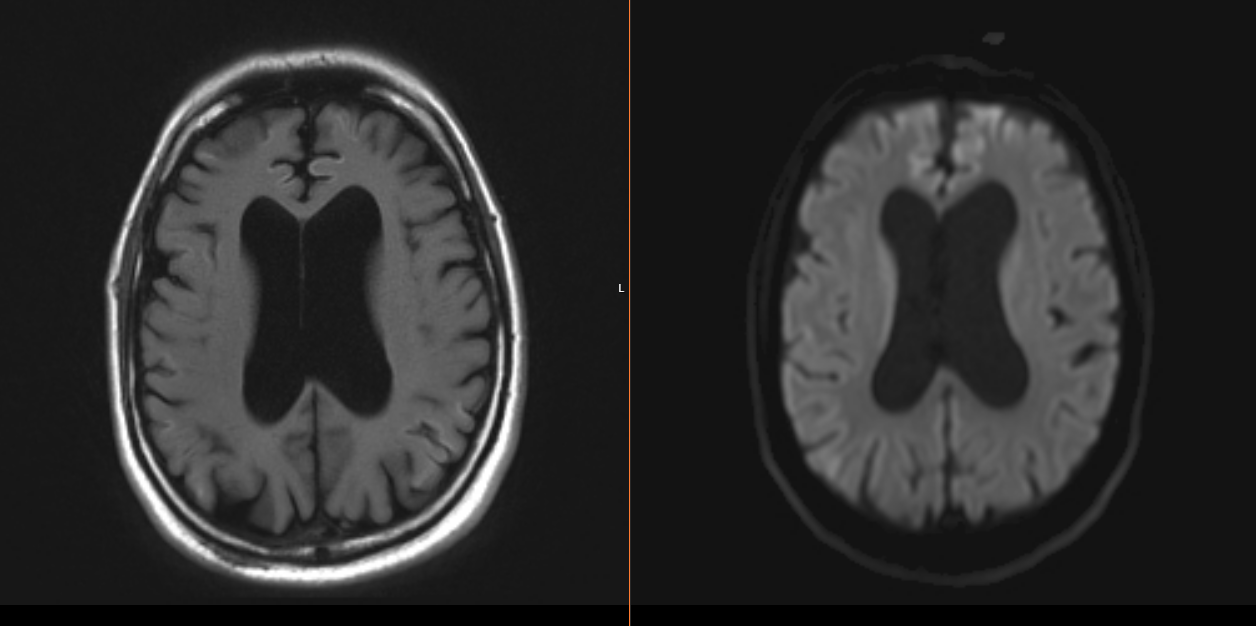
Case Presentation: A 48 y/o man with history of chronic methamphetamine use, schizophrenia, and bipolar disorder presented after being found unconscious associated with urinary incontinence. He was treated for toxic metabolic encephalopathy in setting of sepsis from urinary tract infection and multifocal pneumonia. However, his mental status declined despite initiation of antibiotics. He was alert and oriented to name only. At baseline, he is fully alert and oriented. He was able to follow simple commands with notable expressive aphasia, impaired short-term memory, Argyll Robertson pupils and hyperreflexia. Further questioning from family revealed a one-year rapid decline in his memory and behavior with increasing delusions and visual hallucinations, that acutely progressed two weeks prior to presentation. Given his cognitive decline, he completed a course of methylprednisolone for possible autoimmune encephalopathy without improvement. Infectious workup revealed RPR titer of 1:64 and positive serum treponema pallidum antibody. MRI brain showed diffuse frontal, parietal, and temporal lobe cortical hyperintensity and caudate diffusion. CTA chest displayed large right loculated empyema with chest tube placed for drainage. He underwent a lumbar puncture with negative cerebrospinal fluid (CSF) BioFire but positive CSF treponema pallidum antibody. Repeat RPR titer was 1:128. He started treatment for neurosyphilis with IV Penicillin G. Despite treatment, his mental status did not improve. Electroencephalogram was unremarkable. 14-3-3 CSF titer was elevated (>138,000 AU/mL), with elevated tau protein (>20,000) and indeterminate RT-QUIC. Despite the indeterminate RT-QUIC, neuroimaging findings and extremely elevated 14-3-3 made a diagnosis of Creutzfeldt-Jacob disease (CJD) with neurology evaluation. His empyema was controlled with thoracotomy and decortication.
Discussion: Neurosyphilis can be subdivided into early disease, with findings of asymptomatic neurosyphilis, meningitis, ocular-or oto-syphilis, or late disease with findings of general paresis or tabes dorsalis. The diagnostic criteria for CJD includes progressive dementia, startle myoclonus, visual disturbances, ataxia and akinetic mutism. 14-3-3 are non-specific markers of neuronal injury and have been reported to be elevated in few cases of neurosyphilis, however, the RT-QUIC is a highly sensitive and specific marker for CJD. In our patient’s case, it was indeterminate, but the cortical ribboning on MRI brain coupled with the progressive cognitive decline, visual disturbances and personality changes pointed towards CJD. Typical MRI findings include hyperintense signal on diffuse weighted imaging, fluid-attenuated inversion recovery T2-weighted images involving the cerebral cortex and corpus striatum. Neurosyphilis is known to imitate other pathologies as the “great mimicker” in medicine. However, our case highlights the importance of pursuing a complete workup, with a multidisciplinary team. This led to a diagnosis of CJD, with neurosyphilis as a confounding factor.
Conclusions: This case presented diagnostic difficulties given the multifactorial etiologies of encephalopathy in the setting of infection, psychosis, neurosyphilis, and CJD. Initial testing was consistent with neurosyphilis but considering the lack of symptomatic improvement during treatment, the positive CSF markers of 14-3-3, Tau protein and pathognomonic MRI findings led to the diagnosis of CJD.