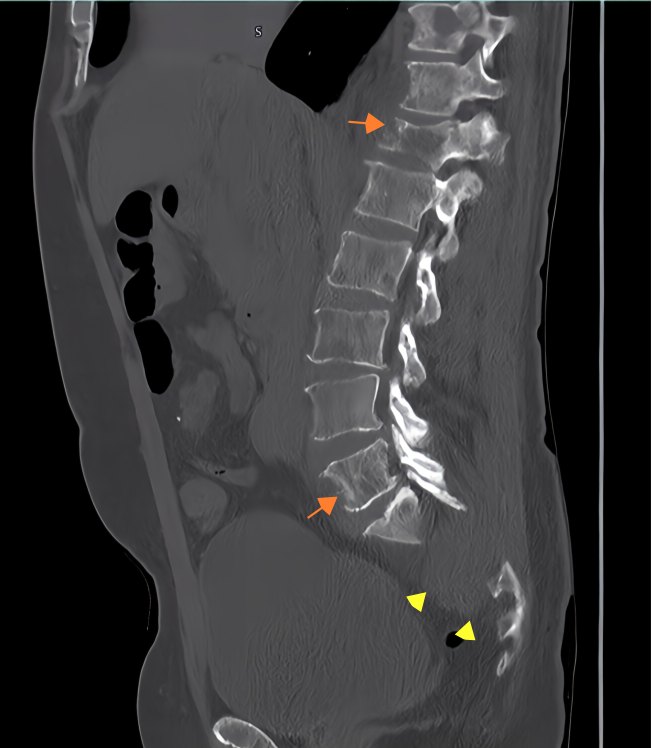
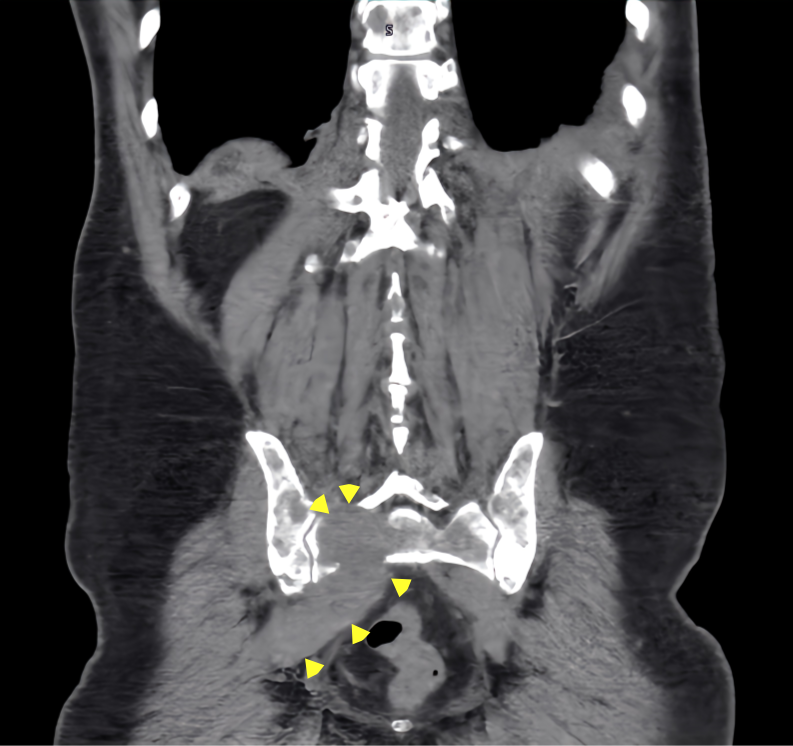
Case Presentation: A 51-year-old male with a history of chronic fentanyl use, smoking (20 pack-years), and occasional alcohol consumption presented with persistent back and flank pain lasting one week. The pain was constant, non-radiating, and accompanied by non-bloody diarrhea. Imaging revealed multiple concerning findings: a large lytic lesion in the right frontal skull (1.9 x 3.1 cm) on a bone survey, a 4.9 x 5.4 x 3.9 cm mass in the right sacrum with diffuse metastatic bone involvement on abdominal and pelvic CT, and T12 compression fractures with sacral involvement on spine MRI. The MRI findings suggested borderline spinal cord compression. Fine needle aspiration (FNA) of the sacral mass confirmed plasma cell neoplasm, with immunohistochemistry positive for CD138 and CD79a. Additional laboratory findings included anemia, elevated creatinine, positive M-protein isotype, increased Lambda free light chains, and a decreased Kappa/Lambda ratio. Initially considered an isolated lesion, the sacral mass was ultimately identified as part of a systemic multiple myeloma (MM) process. The patient was diagnosed with MM and referred to radiation oncology for further management.
Discussion: This case underscores the importance of including malignant spinal tumors, such as solitary plasmacytoma (SP), in the differential diagnosis for patients presenting with persistent back pain unresponsive to conservative treatment. SP, though rare, is clinically significant due to its potential to progress to MM. This progression highlights the necessity of prompt and accurate diagnosis. Imaging modalities like MRI and CT are essential for identifying spinal lesions and differentiating SP from other spinal pathologies, such as degenerative changes or metastatic disease. FNA, supported by immunohistochemical analysis, offers a minimally invasive method for confirming plasma cell neoplasms. Radiotherapy remains the cornerstone of treatment for localized SP, aiming to control symptoms and prevent further disease progression. However, as this case demonstrates, systemic involvement can masquerade as localized disease, emphasizing the need for a comprehensive diagnostic approach, including bone surveys and laboratory evaluation of systemic markers.
Conclusions: This case highlights the challenges of diagnosing plasma cell neoplasms with unusual presentations, such as sacral involvement initially mimicking solitary plasmacytoma. The findings underscore the critical role of advanced imaging and biopsy in the diagnosis of SP and MM. Early recognition and intervention are key to improving outcomes, as localized SP carries a better prognosis compared to MM. This case also illustrates the importance of considering systemic disease even in cases with initially localized findings, thereby reinforcing the need for a multidisciplinary approach in managing plasma cell neoplasms.