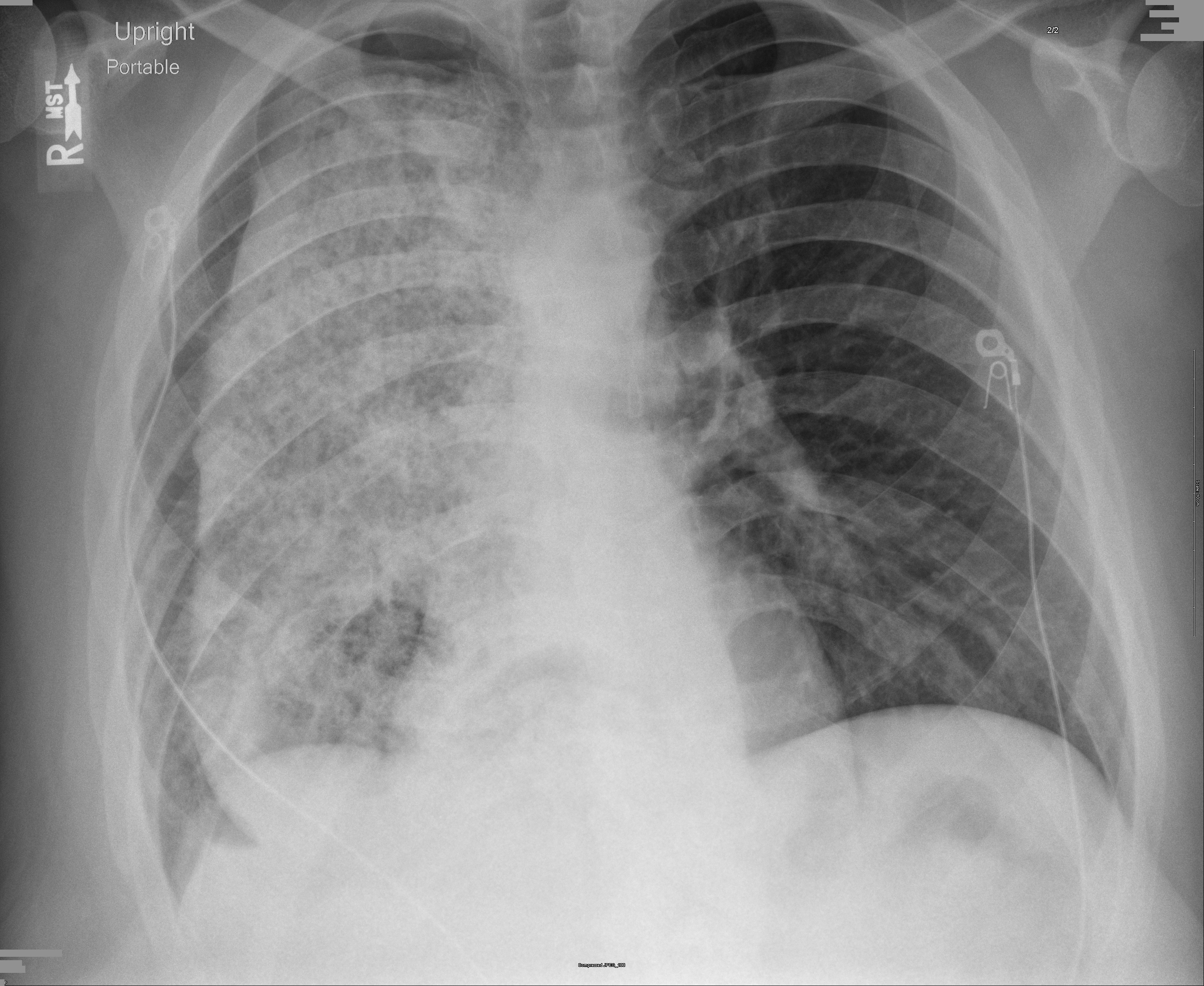
Case Presentation: We report a case of a 38-year-old African American male with history of dysphagia who presented with complaint of acute chest pain. He described it as pressure like mid-sternal chest pain, radiating to his left arm associated with palpitations, worse on exertion and diaphoresis. On presentation, he was found to have atrial fibrillation with rapid ventricular response (RVR). His Chest X-ray revealed more than 80% diffuse opacification of right sided lung field, with smooth margins. Patient was admitted to the hospital service for management of chest pain, atrial fibrillation with RVR and possible lung infiltration. During further evaluation patient reported of having 50lbs weight loss over past 6 months and undergoing an unknown stomach surgery 5 years ago for acid reflux. CT scan of the chest revealed marked dilation of the esophagus with a large amount of debris, causing mass effect and volume loss of the right lower lobe. Due to the severity of esophageal distension, thoracic surgery was consulted for surgical intervention for end stage achalasia. Thereafter, patient underwent McKeown esophagostomy with cervical esophagogastrostomy, partial proximal gastrectomy, intercostal nerve cryo-ablation and feeding jejunostomy. Post-op patient had a quick recovery and atrial fibrillation reverted back to sinus rhythm.
Discussion: Chest pain is the second most common complaint amongst patients visiting ED, resulting in approximately 6 million annual visits in the US. Atrial fibrillation (AF) is the most common cardiac arrhythmia, accounting for an estimated 2.7-6.1 million people in the US. Patients with AF are at increased risk for death, heart failure, hospitalization and thromboembolic events. Long-term AF-related stroke and mortality risks have found be similar between individual with and without secondary, or reversible, AF precipitants. Achalasia, an uncommon condition, results from progressive degeneration of ganglion cells in the myenteric plexus in the esophageal wall, leading to failure of relaxation of the lower esophageal sphincter along with loss of peristalsis in the distal esophagus. It has an insidious onset with gradual progression of symptoms. Hence, it usually does not make it to the top of differential diagnosis for acute chest pain and atrial fibrillation. However, Achalasia is one of the rare disorders which, if left untreated, can present with acute chest pain and atrial fibrillation; and can potentially increase long-term AF-related stroke and mortality risks.
Conclusions: Acute onset of chest pain and atrial fibrillation can result from a broad spectrum of disease process. Thus, having a systematic approach to the broad differential can efficiently decrease the risk factors associated with the disease process.