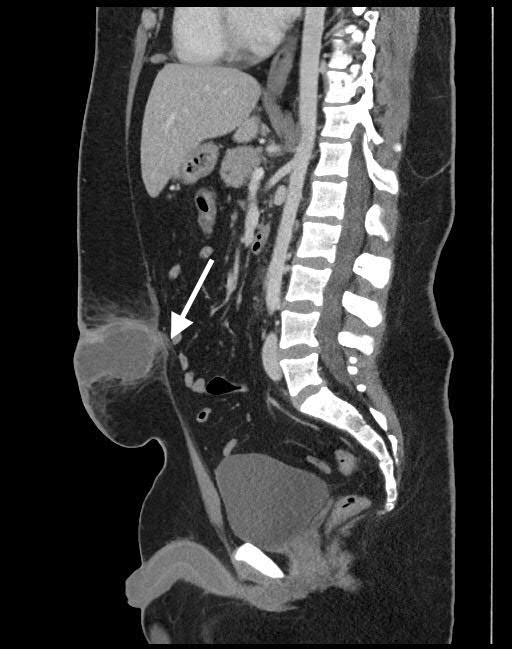
Case Presentation: A 19 year-old obese man presented to the emergency room with 5-day history of periumbilical rash, pain and bloody purulent umbilical discharge.On presentation, the patient was febrile (38.4 C), hypotensive (98/54 mmHg), and tachycardic (111 beats/min). On exam, the periumbilical region was erythematous, indurated, and tender to palpation without rebound tenderness or guarding.Laboratory study revealed leukocytosis (12.4 x 10^9/L). Serum lactate and creatinine were normal. Contrast-enhanced computed tomography (CT) of the abdomen showed a 6 x 4 x 4 cm lobulated subcutaneous umbilical abscess. The posterior aspect had a beak like connection to the top of the urachus suggesting an infected urachal sinus (figure 1). He received intravenous (IV) fluid and broad-spectrum IV antibiotics prior to being admitted to medicine service for management of periumbilical cellulitis and infected urachal remnant. On admission, the patient underwent urgent ultrasound-guided drainage and drain placement. Urology recommended Foley catheter placement for bladder decompression due to concern for a patent urachal remnant. Patency was later ruled out given a normal creatinine level from the fluid collection. Cultures had polymicrobial growth. The patient improved clinically with treatment and was discharged with the abdominal drain and IV antibiotics on hospital day 5. The drain was removed 4 days post discharge after an outpatient sinogram showing resolution. He received 2-week IV antibiotic therapy followed by amoxicillin-clavulanic acid for prophylaxis. Five weeks after discharge, he underwent successful surgical excision of the urachal remnant with umbilical reconstruction (figure 2). Pathology showed fibrosis and chronic inflammation.
Discussion: The urachus is an embryologic tract that extends from the bladder to the umbilicus during fetal life. The tract involutes around birth forming the median umbilical ligament. Incomplete involution results in 4 types of urachal anomalies: patent urachus, umbilical-urachal sinus (our patient), vesicourachal diverticulum, and urachal cyst. The incidence of urachal remnants is 1% of the population. Owing to the low incidence and non-specific signs and symptoms, infected urachal remnants may be misdiagnosed leading to therapeutic failure and recurrence. Common presenting symptoms include abdominal pain, umbilical discharge, periumbilical erythema, fever, and midline mass. Infected urachal remnants can be accurately demonstrated by ultrasound or CT scan. Differentiating urachal carcinoma from infection based on imaging can be difficult. To assess urachal potency, radiocontrast can be injected into the urachal opening at the umbilicus. Alternatively, fluid creatinine level from the urachus can be measured to detect the presence of urine. The treatment of infected urachal remnants involves antibiotics, drainage, followed by excision of the remnant to prevent recurrence of infection and future development of malignancy.
Conclusions: 1. The urachus is a tract that connects the bladder to the umbilicus during fetal life. Incomplete involution results in urachal anomalies.2. Umbilical discharge, midline abdominal mass, and abdominal pain should raise suspicion for urachal anomalies. 3. Due to low incidence and non-specific signs and symptoms, infected urachal remnants may be misdiagnosed leading to therapeutic failure and recurrence.4. Treatment involves antibiotics, abscess drainage, followed by excision of the remnant.