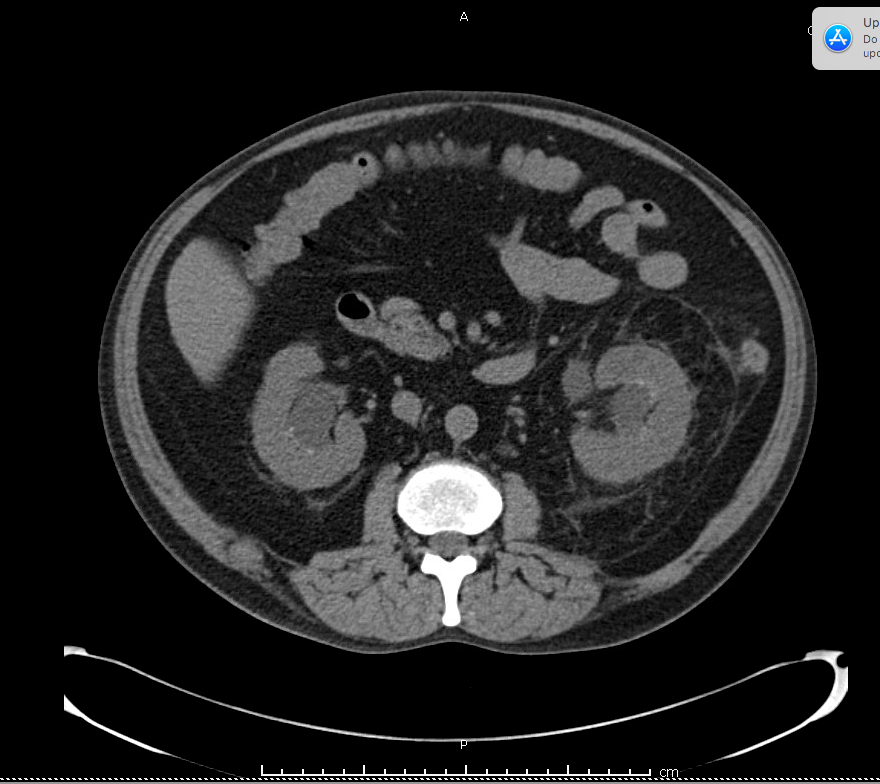
Case Presentation: A 60 year old male with history of diverticulitis, uric acid nephrolithiasis, gout presented with 1 day history of sudden onset left lower quadrant pain and decreased urine output. Pain was a constant aching pain that radiated to his left flank and was gradually worsening. Since symptom onset, patient also reported scant urine output with no urge to go. Bowel movements and oral intake had been normal prior to symptom onset. He had otherwise been in his usual state with no fevers, chills, malaise or weight changes. His last episode of diverticulitis was 3 months prior and was treated medically. Uric acid stones were non-obstructive and he had never required any intervention. Home medications were allopurinol, metformin, and losartan. Exam was significant for tenderness in the left lower quadrant without peritoneal signs and bilateral flank tenderness. Labs showed leukocytosis to 21, creatinine of 5 from 1.3 prior, and uric acid of 12.2. Imaging showed bilateral kidney stones obstructing the ureters at the same level with resulting hydroureter and perinephric fat stranding. He was taken immediately by urology for ureteroscopy and bilateral stent placement. Following stent placement, patient had post-obstructive diuresis with gradual improvement of kidney function but continued to have significant left lower quadrant pain and poor oral tolerance. Repeat CT ultimately showed uncomplicated sigmoid diverticulitis and patient was medically managed with resolution of symptoms.
Discussion: Occam’s razor is a commonly used principle where clinicians attempt to find the simplest single diagnosis to unite a patient’s multitude of symptoms. However, there can be times when a patient truly has multiple disease processes simultaneously that can be missed when creating a unifying diagnosis. In this patient’s case, nephrolithiasis was initially thought to be the explanation for his symptoms and led to a delayed diagnosis of his diverticulitis. This case highlights the limitations of using occam’s razor and emphasizes the importance of frequent re-evaluation during the diagnostic process. Although a single diagnosis is often correct, one must always have a high clinical suspicion for additional processes so as not to miss other diagnoses. Nephrolithiasis is relatively common with a lifetime risk of ~12% in men and 6% in women. Bilateral ureteral stones, though, are relatively uncommon and resulting acute kidney injury is even more rare, only documented in a few case reports. However, acute renal failure as a complication of stones is important to recognize as it requires immediate urological intervention to prevent long-lasting kidney damage.
Conclusions: Bilateral kidney stones are a rare but significant cause of acute kidney injury that must be recognized promptly by the general internist. Additionally, it is important for clinicians to be aware of the limitations of Occam’s razor and reevaluate frequently to appropriately diagnose a patient.