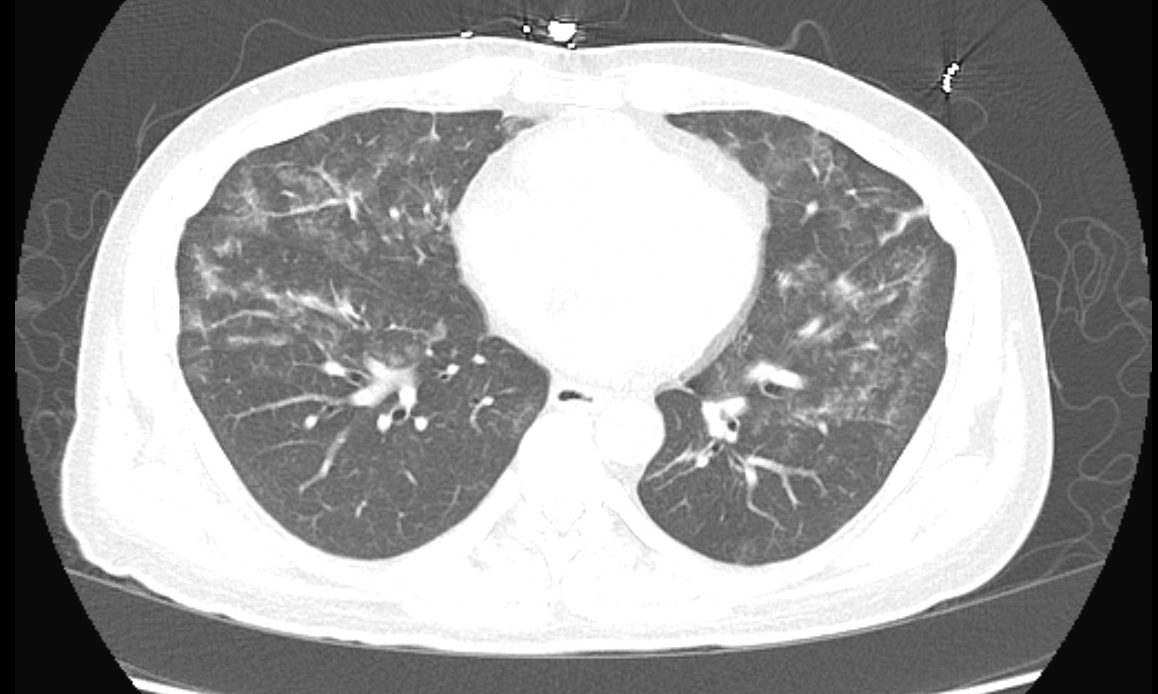
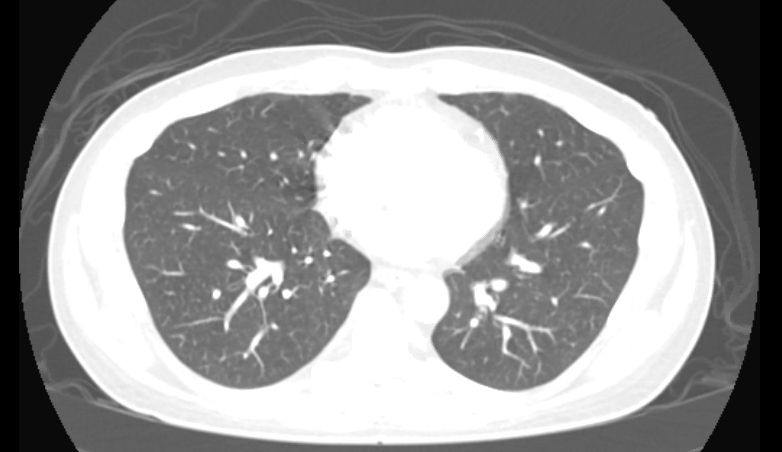
Case Presentation: A 47 year old man with asthma and a 30 pack-year smoking history presented with shortness of breath, chest tightness, and intermittent fevers for the past week. For the month prior to presentation he was vaping tetrahydrocannabinol (THC) daily. He had no sick contacts and no other drug use or occupational exposures. Initial vital signs were normal with an oxygen saturation of 97% on room air. Soon after admission he was febrile to 38.9 C and remained persistently febrile for over 24 hours. Physical exam was notable for clear lungs bilaterally. Labs were remarkable for a white blood cell count of 12.2×10^9 cells/L with 86% neutrophils, elevated erythrocyte sedimentation rate of 70 mm/hr, and elevated C-reactive protein at 24.43 mg/dL. Remaining labs including sputum culture, blood cultures, respiratory viral panel, Streptococcus pneumoniae and Legionella pneumophila urinary antigens, HIV, ANA, p-ANCA, and c-ANCA were all negative. Initial chest x-ray was normal; however, chest CT demonstrated diffuse bilateral ground-glass opacities. He was started on ceftriaxone and azithromycin due to concern for community-acquired pneumonia. Given his clinical presentation and risk factors he was diagnosed with e-cigarette, or vaping, product use associated lung injury (EVALI) and started on a prednisone taper in consultation with the pulmonary team. He was discharged home on a prednisone taper as well as cefpodoxime and azithromycin. Repeat chest CT two weeks later demonstrated complete resolution of the diffuse bilateral ground-glass opacities.
Discussion: Fever and shortness of breath are common presenting symptoms evaluated by practicing hospitalists. Usually, this presentation represents pneumonia; however, a thorough social history and consideration of vaping exposure are necessary given the similar clinical presentation of EVALI. As of November 21, 2019, there have been 2,290 cases of EVALI reported to the Centers for Disease Control (CDC). Of the cases in which symptoms were reported, 85% had respiratory symptoms (cough, chest pain, shortness of breath), 76% had constitutional symptoms (fevers, chills, weight loss), and 57% had gastrointestinal symptoms (abdominal pain, nausea, vomiting, diarrhea). The majority of these cases (83%) were associated with THC-containing product use in the three months prior to symptom onset. All patients with reported imaging findings had abnormal chest CTs with almost all (96%) having abnormalities visualized bilaterally. Interestingly, among those who had both a chest x-ray and CT chest, 38% had a normal chest x-ray but abnormal chest CT as was demonstrated in our case. EVALI is a diagnosis of exclusion and may co-occur with and be difficult to distinguish from respiratory infections such as pneumonia therefore treatment may include empiric antimicrobials. The majority of patients with EVALI who have received corticosteroids have demonstrated rapid improvement. Finally, patients should be counseled to discontinue use of e-cigarette or vaping products.
Conclusions: EVALI is a newly recognized condition that is important for clinicians to consider, particularly in patients with respiratory, gastrointestinal, or constitutional symptoms. It is important for clinicians to ask patients about e-cigarette and vaping product use and maintain a high index of suspicion for EVALI in the appropriate clinical context even if the initial chest x-ray is normal. Clinicians are encouraged to report cases of EVALI to their local or state health departments.