Background: Large volume preparations that are polyethylene glycol based (such as GoLYTELY and MiraLAX) are the mainstay of bowel preparation regimens at many institutions. Studies have shown that patients prefer lower volume preparations compared to the standard 4 Liters of polyethylene glycol electrolyte solutions (PEG- ELS). Although data has been collected on low volume bowel preparation efficacy in the outpatient setting for elective colonoscopy, there is scant data on low volume bowel preparations in the inpatient setting. We performed a retrospective review of patients who received Clenpiq (sodium picosulfate, magnesium oxide, and anhydrous citric acid), a low volume bowel preparation for colonoscopies at our institution.
Methods: A retrospective review from the past year (2019-2020) was done to assess which patients underwent bowel preparation with Clenpiq (sodium picosulfate, magnesium oxide, and anhydrous citric acid) at a single institution. On the evening prior to the colonoscopy, patients were instructed to drink 2 bottles of Clenpiq (160 mL solution) six hours apart. Each bottle was followed by 32 oz ounces of clear liquids. All patients, age greater than 18 who did not meet exclusion criteria were included in the study. Exclusion criteria included patients with severe renal impairment (CrCl < 30 mL/min), GI obstruction or ileus, bowel perforation, colitis, gastric retention, hypersensitivity to compounds of formula.
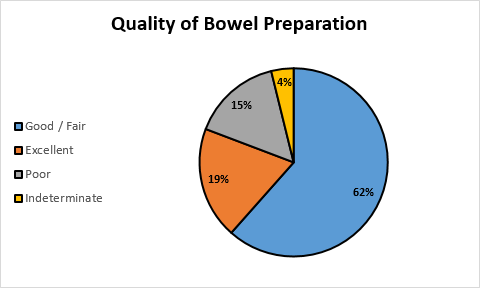
Results: 37 patients were scheduled to receive low volume bowel preparation. 11 of these patients were excluded from the study due to leaving the hospital prior to having the procedure. 26 patients (6 Males, 20 Females, mean age = 57.2) were ultimately analyzed. 24 out of the 26 patients finished the bowel prep in its entirety (92.3%). 4 out of the 26 patients experienced adverse reaction of nausea (15.4%). Of the 4 patients who experienced nausea, 2 were unable to finish the prep. 5 out of the 26 patients had an excellent bowel preparation as determined by the endoscopist using the Boston Bowel Prep Scale (BBPS; score = 9; 19.2%). 16 out of the 26 had at least fair or good bowel preparation as determined by the endoscopist using the BBPS (score = 6, 61.5%), while 4 patients had poor quality bowel prep (15.4%). 0 cases needed to be rescheduled due to inadequate bowel preparation. The most common indications for colonoscopy were anemia, hematochezia, abdominal pain, and abnormal imaging.
Conclusions: The inpatient setting is associated with increased comorbidities and conditions that can prevent proper preparation, and there is currently no standardized bowel preparation type for the inpatient setting. The inpatient setting compared with the ambulatory setting, has been associated with almost a two-fold higher risk of inadequate bowel preparation prior to colonoscopy. Inadequate bowel preparation is associated with increased risk of missed lesions, resulting in repeat and lengthier procedures. Although PEG-ELS preparations are well tolerated, many patients do not complete the bowel preparation due to the large volume required. From our limited data, the majority of patients that took Clenpiq prior to colonoscopy, were able to fully finish the prep, had adequate prep and were able to tolerate it without any adverse reactions. As a result of the COVID-19 pandemic, and major limitations on elective cases, we will pursue prospective analysis of cases in the future. Further research should be done to compare Clenpiq with GoLYTELY as an alternative to routine bowel prep in hospitalized patients.