Background: Prior studies of routine blood culture (BC) testing in uncomplicated community acquired pneumonia (CAP), skin and soft tissue infections (SSTI), and urinary tract infections (UTI) have demonstrated low utility given similar rates of pathogen versus contaminant detection and little effect on clinical management. Understanding patterns and outcomes of BC testing can identify opportunities to curb unnecessary testing.The objectives of this study were to: 1) Evaluate BC testing trends over time for children hospitalized for CAP, SSTI, and UTI; and 2) measure differences in clinical outcomes among hospital groups with low, moderate, and high testing rates.
Methods: We conducted a retrospective cohort study using the Pediatric Health Information System database to identify hospitalizations for patients aged 3 months to 18 years admitted with CAP, SSTI, or UTI from 2016-2023. We excluded encounters for complicated disease (e.g., empyema, necrotizing fasciitis), complex chronic conditions, ICU admission, or length of stay (LOS) >7 days. We examined hospital-level BC rates by infection type, averaged across the entire time period, and changes in annual BC testing over time by hospital, identified by logistic regression. Using k-means clustering, we grouped hospitals into low, moderate, and high BC testing groups based on similarities of BC testing rates in the aggregate of the 3 study infections. We compared LOS, costs, and ED revisits across testing groups using generalized estimating equations adjusted for condition, age, and H-RISK severity.
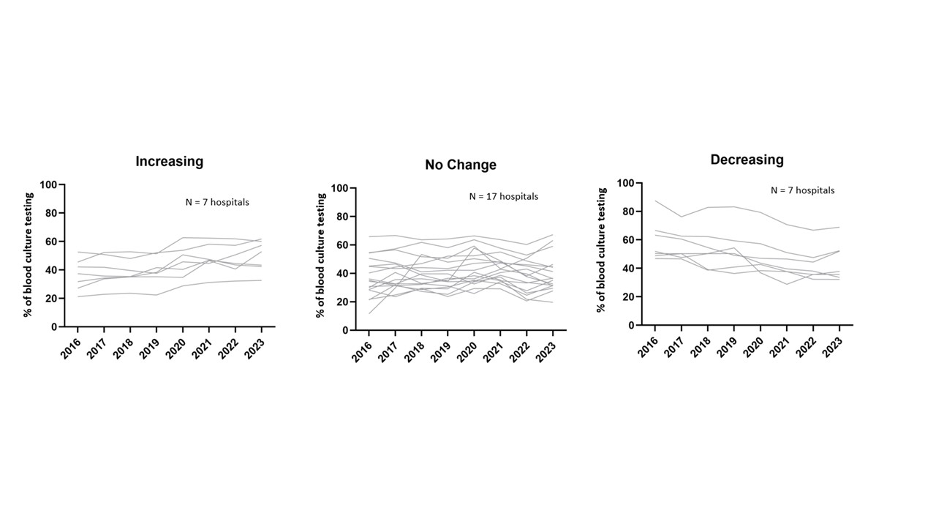
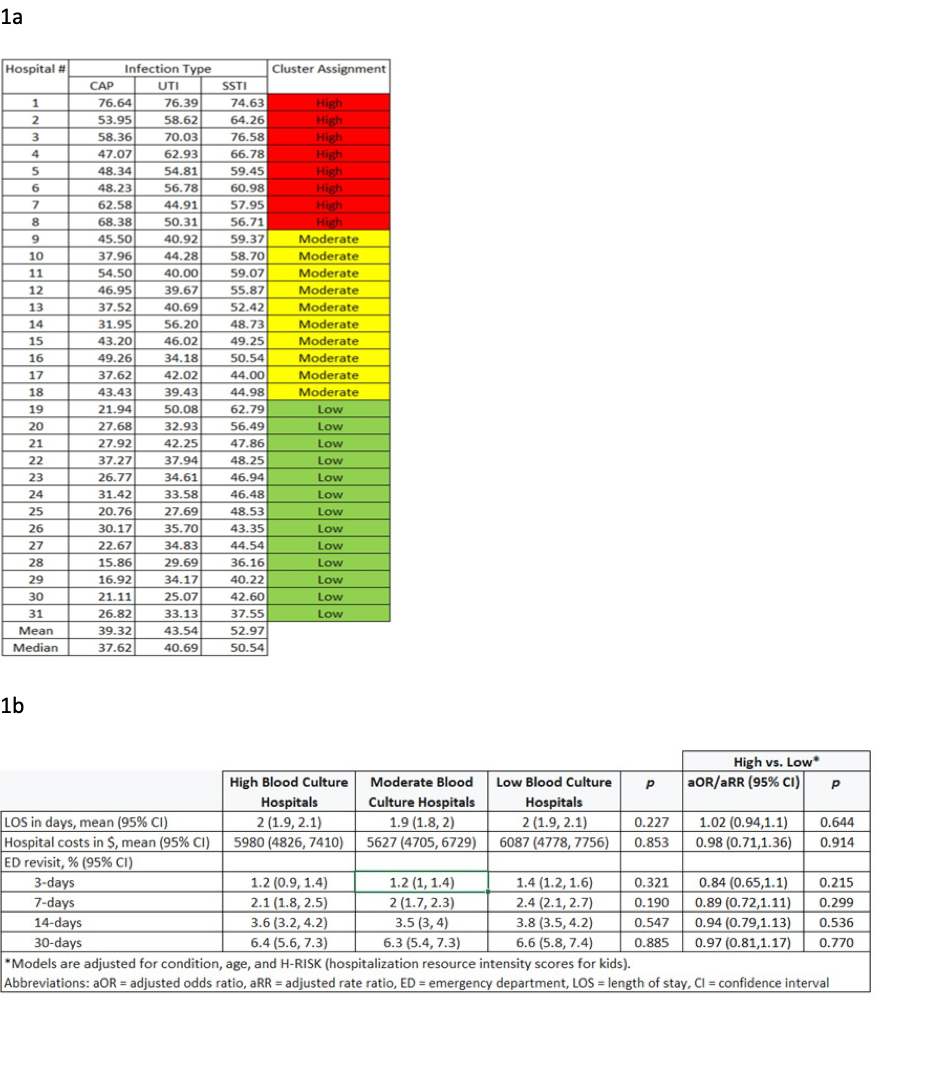
Results: We identified 94,524 hospitalizations across 31 hospitals; BCs were obtained for 41% of CAP, 45% of SSTI, and 55% of UTI encounters. Hospital-level use of BCs varied widely across all 3 infections (e.g., CAP: 16% to 77%; Table 1). Trends over time showed 7 hospitals with statistically significant increases in annual testing while 7 demonstrated decreases in annual testing (Figure 1). Clustering resulted in 13 hospitals in the low, 10 in the moderate, and 8 in the high BC testing groups (Table 1a). There were no significant differences in adjusted costs, LOS, or ED-revisits across BC testing groups (Table 1b).
Conclusions: Among a large cohort of children admitted with CAP, SSTI, and UTI, BC testing rates remain high with substantial variation across hospitals. Many hospitals demonstrated no change or an increase in BC testing trends despite mounting evidence discouraging this practice. With current national shortages in culture supplies and to provide best evidence-based care, it is critically important to evaluate blood culture practices and identify opportunities for safely reducing blood culture use.