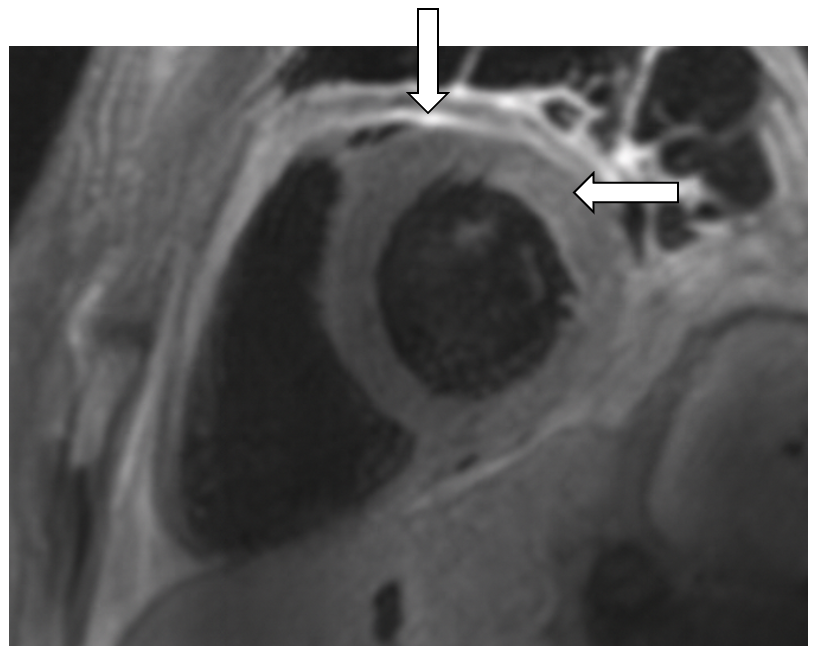
Case Presentation: A 24-year-old woman with type IV glycogen-storage disease and liver transplant presented with fevers, pleuritic chest pain, and odynophagia. On exam, she had multiple ulcers in the posterior pharynx and on bilateral labia majora. Laboratory studies showed elevated NT-proBNP (2717), troponin (367), and CRP above assay (>300). ECG demonstrated nonspecific ST elevations and depressions. CT angiography did not demonstrate intrathoracic pathology. She was admitted to hospital medicine. Swabs from oral and vulvar ulcers were positive for herpes simplex virus 1 (HSV-1) on polymerase chain reaction (PCR), and we initiated IV acyclovir due to concern for disseminated infection. Transthoracic echocardiography (TTE) demonstrated pericardial thickening and effusion, consistent with pericarditis. We added colchicine and indomethacin, and cardiac MRI confirmed acute myopericarditis with constrictive pathology (Figure 1). By hospital day 4 (HOD4), she developed dry cough, 2+ lower extremity edema, and weight gain, which resolved with diuresis. We pursued a broad infectious work up for myopericarditis; however, serum testing for HSV-1/2, Epstein-Barr virus, cytomegalovirus, and coxsackie were negative. By HOD9, her chest pain and odynophagia improved, and repeat TTE demonstrated improving myopericarditis. We deferred myocardial biopsy. We discharged her on oral valacyclovir, indomethacin, and colchicine for ongoing treatment of HSV myopericarditis with close follow-up with cardiology and infectious disease.
Discussion: HSV is a rare cause of acute myopericarditis, cited in only a few case reports. In this patient, serum HSV-1/2 PCR was negative despite evidence of disseminated infection. This is consistent with prior case reports in which clinical syndrome, serology, and serum PCR are not well correlated thus requiring tissue diagnosis. In one published case, HSV infection led to fulminant myocarditis and death despite PCR-negative serum testing and was only identified in the myocardium upon autopsy [1]. In our patient, myocardial biopsy was deferred due to high clinical suspicion of HSV-related disease combined with her marked clinical improvement with IV acyclovir. Regardless of serology and serum testing, disseminated ulcerative lesions must raise suspicion for HSV myopericarditis. The gold standard for diagnosis of myopericarditis is endomyocardial biopsy [2]. However, clinical diagnosis through laboratory studies, ECG, echocardiography, and cardiac MRI is essential due to the invasive nature of endomyocardial biopsy. The mainstays of treatment are NSAIDs with taper over 3-4 weeks, as well as colchicine to decrease rates of recurrence [3]. With myocardial involvement, additional management may include diuretics, as in our patient’s case, and in some cases, advanced heart failure therapies [3].
Conclusions: HSV is a rare cause of acute myopericarditis with high morbidity that requires a high level of clinical suspicion for diagnosis. Our case illustrates the importance of prioritizing HSV on the differential for myopericarditis, especially in immunosuppressed patients, as it can have potentially lethal consequences if left untreated or missed.