Background: Hispanic patients consistently experience higher risk of hospital admissions, driven by structural barriers such as lower health literacy, limited English proficiency (LEP), and reduced access to timely outpatient care. There had been system-level initiatives such as Hospital Readmission Reduction Program (HRRP), and individualized, culturally tailored care transition programs (Mi Puente), but none has been successful in addressing higher readmission rates specific to this vulnerable population. Recently, a post-discharge Virtual Transition of Care (VToC) clinic pioneered by our hospitalist group showed great promise in reducing readmission amongst discharged patients from the hospital medicine service. However, its impact on patient populations at disproportionate risk, including racial, ethnic, language preference and insurance subgroups, warrants further investigation. The objective of this study is to determine whether the impact of VToC on 30-day readmissions among Hispanic patients differs by language preference and insurance status.
Methods: We conducted a retrospective sub-analysis of the UC San Diego Health VToC cohort (September 2021 to September 2024, N=8143). Hispanic patients discharged alive and all eligible discharges from patients with multiple hospitalizations were included; those with planned admissions were excluded. The intervention group completed a VToC visit within seven days of discharge. Controls included those without VToC attendance. Primary outcome was all-cause 30-day unplanned readmission. Analyses were stratified by insurance (government vs non-government) and language (English vs non-English preferring). Outcomes were compared using 2×2 contingency tables, and absolute risk difference (ARD), crude odds ratios (OR) with 95% confidence intervals (CI), along with P values were calculated.
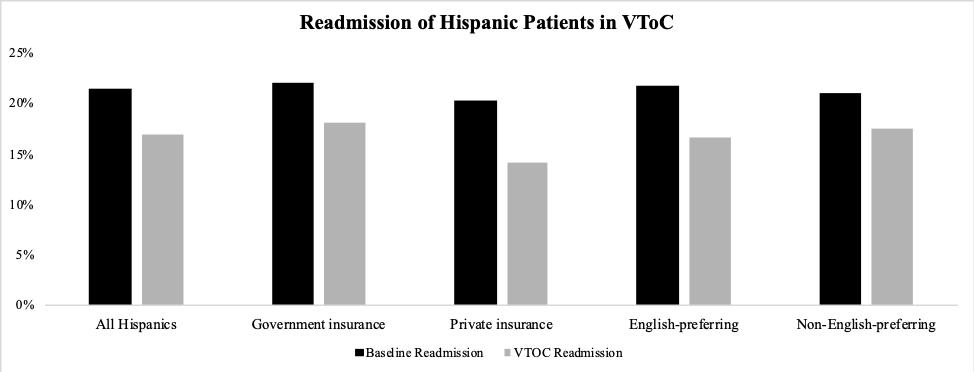
Results: The 30-day readmission rate for Hispanics who participated in VToC was 16.9% (143/844), significantly lower than the 21.3% (1556/7299) observed in the benchmark group (p< 0.003). Privately insured (ARD –6.12%, OR 0.64, 95% CI 0.44 – 0.97, p< 0.03) and English-preferring (ARD –5.05%, OR 0.72, CI 0.56 – 0.93, p< 0.01) patients had the strongest benefits. Government insured (ARD –3.90%, OR 0.78, 95% CI 0.63 – 0.97, p< 0.03) patients had less, but still statistically significant benefit. Spanish-preferring showed a directionally protective, otherwise non-significant reduction (OR 0.80, 95% CI crossing 1, p=0.135).
Conclusions: VTOC was associated with a significant reduction in unplanned readmissions among high-risk Hispanic patients, with the strongest effect in the English-preferring and privately insured subgroup. In contrast, the non-English-preferring patient subgroup did not experience a statistically meaningful reduction. This uneven impact across language and insurance strata suggest that while having close post-discharge follow-up such as VToC is effective, it is insufficient on its own for populations facing confounding structural and systemic to care in the vulnerable period immediately after hospitalization. As a hospitalist-led program, these results reveal an important opportunity for hospitalists to expand their influence beyond hospital walls by actively identifying upstream confounders and engaging with the appropriate resources early. By doing so, hospitalists can play a vital role in driving efforts in the care continuum to close gaps that disproportionately affect disadvantaged populations.