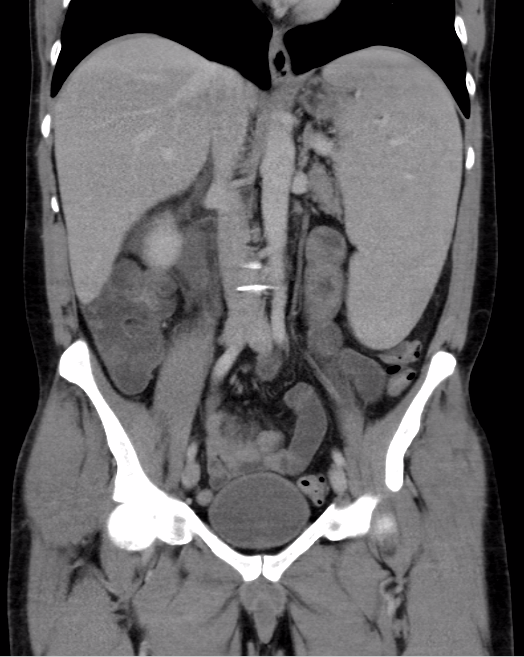
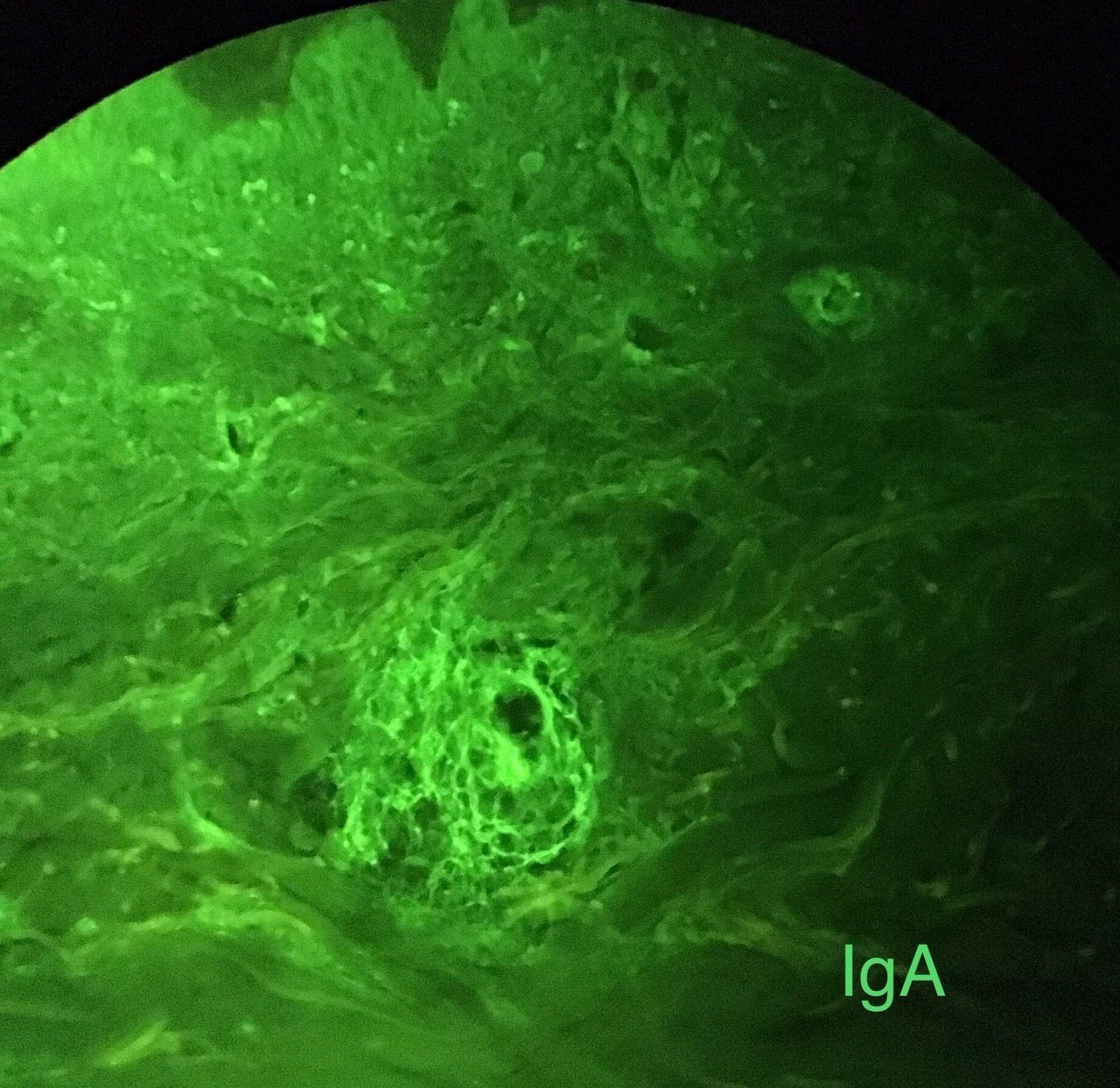
Case Presentation: A 50-year-old man without significant medical history presented with two months of purpura over his lower extremities and abdomen, ankle pain, and two days of severe abdominal pain associated with vomiting and melena. His symptoms started following a respiratory infection. On presentation, he was afebrile with normal vital signs. Physical exam was notable for a tender abdomen and non-blanchable purpura of his lower extremities to the thighs and across his abdomen.Laboratory testing demonstrated chronic lymphopenia (WBC 2.4×109 cells/L), microcytic anemia (hemoglobin of 12 g/dL, MCV 78.3 fL), and normal platelets. His serum creatinine was 1.1 mg/dL and urinalysis was negative for blood and protein. Complements were normal. Inflammatory markers were elevated (CRP of 45 mg/L and ESR of 43 mm/hr). Blood cultures were negative. CT abdomen demonstrated a 23 cm spleen and duodenal thickening without lymphadenopathy. No splenic vein thrombosis was visualized. HIV, HBV, HCV, EBV, ANA, RF, and anti-CCP were negative. cANCA was slightly positive (titer 1:80) but with negative PR3 and MPO. SPEP and UPEP were without significant abnormalities. Punch biopsy demonstrated leukocytoclastic vasculitis and immunofluorescence showed IgA deposition. EGD revealed large, circumferential patches of ulcerated, friable mucosa in the duodenum. Histology was consistent with acute inflammation and immunohistochemical stains for CMV and HSV were negative. Given a negative infectious workup, the patient started oral prednisone for presumed IgA vasculitis with rapid symptom improvement. Splenomegaly persisted after discharge prompting a peripheral smear which was concerning for hairy cell leukemia. He was referred for bone marrow biopsy, which did not reveal underlying malignancy by histology, cytogenetics, or flow cytometry.Given concern for isolated splenic lymphoma, a PET scan was obtained, but no splenic uptake was seen. He remains asymptomatic after weaning steroids and serial imaging demonstrates improvement in his splenomegaly to 17 cm.
Discussion: IgA vasculitis (IgAV) classically presents with palpable purpura, abdominal pain, arthralgias, and renal disease. Our patient lacked renal disease, which occurs in approximately one third of adult cases (1). He had massive splenomegaly which has not been described as a feature of adult-onset IgAV. The differential diagnosis for massive splenomegaly is limited, including lymphoma, leukemia, myelofibrosis, beta-thalassemia, malaria, leishmaniasis, sarcoidosis, and some HIV-associated infections (2). Given the association between malignancy and IgAV, our patient underwent a thorough investigation for neoplastic causes which was negative. Although the differential for massive splenomegaly is narrow, there are cases where the etiology remains idiopathic. Splenectomy studies to evaluate etiology in such cases ultimately diagnosed most with neoplastic disease, however up to 33% of cases remained idiopathic (3). Such cases require surveillance and discussion of splenectomy with the patient.
Conclusions: Purpura, arthritis, and abdominal pain should drive suspicion for malignancy-related vasculitis and initiate specialty consultation for diagnosis and management. This unusual case with splenomegaly hints at underlying neoplasm, however the etiology remains idiopathic. Given the interval decrease in spleen size, the patient has opted to be followed with serial splenic imaging rather than diagnostic splenectomy.