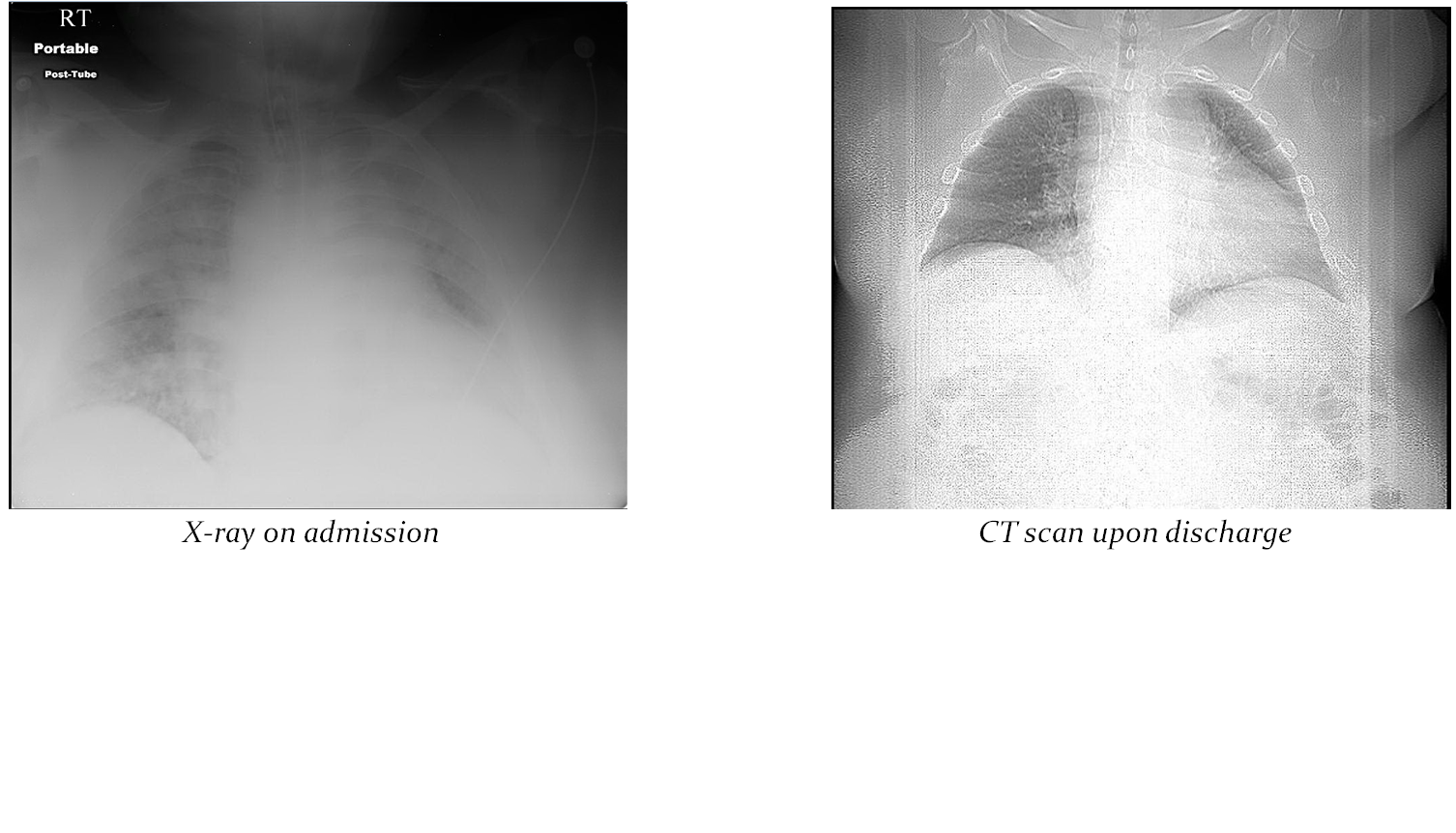
Case Presentation: A 54-year-old morbidly obese male, with a history of asthma, hypertension, bilateral knee replacement and tobacco abuse was found unresponsive outside his home on Christmas Eve. EMS brought him with severe hypercapnic respiratory failure pC02 99.7, white count 21 X 103/mcL, cocaine screen positive and blood ethanol level of 0.230 g/dl. Initial chest x-ray demonstrated bilateral interstitial and airspace consolidation. The patient was intubated and started on coverage for aspiration pneumonitis. Sputum cultures were positive for 1+ Enterobacter cancerogenus and 1+ Pantoea agglomerans. Oerskovia species were reported in 2 of 2 sets of blood cultures. Susceptibilities were sent to an outside lab for further study. Literature review of preliminary culture results linked this bacterium to prosthetic material infections. Bactrim was initiated and knee x-ray found a small right knee effusion.
The patient’s mental status improved, and he was successfully extubated. Antibiotics were modified with the addition of Ampicillin-Sulbactam. The patient was transferred to the medical floor and was discharged with last memory of drinking one bottle of tequila at a Christmas party before coming to the hospital.
Discussion: When the culture report reads, “Possible contamination, clinical correlation is recommended” it is understood that an unusual organism has been cultured. Knowing that equivocal culture results often lead to diagnostic uncertainty and are associated with poor outcomes and increased costs; it is imperative to determine whether the organism is just a contaminate or pathogenic in this situation. Multiple factors are considered including: (1) immunosuppression (2) comorbidities, (3) drugs or alcohol, (4) environmental concerns, (5) type of infection, (6) type of culture, and (7) whether or not the organism is a commonly identified contaminate.
In our patient, this process lead us to conclude that a surprisingly uncommon organism (Oerskovia) was the source of sepsis, but the exact mechanism of infection remained unclear.
Conclusions: Our patient was at increased risk of developing aspiration pneumonia due to alcohol and drug use. His morbid obesity and presumptive obesity hypoventilation syndrome may have contributed to the hypercapnia. Aspiration pneumonias are notorious for being polymicrobial; however, Oerskovia would not be an expected organism.
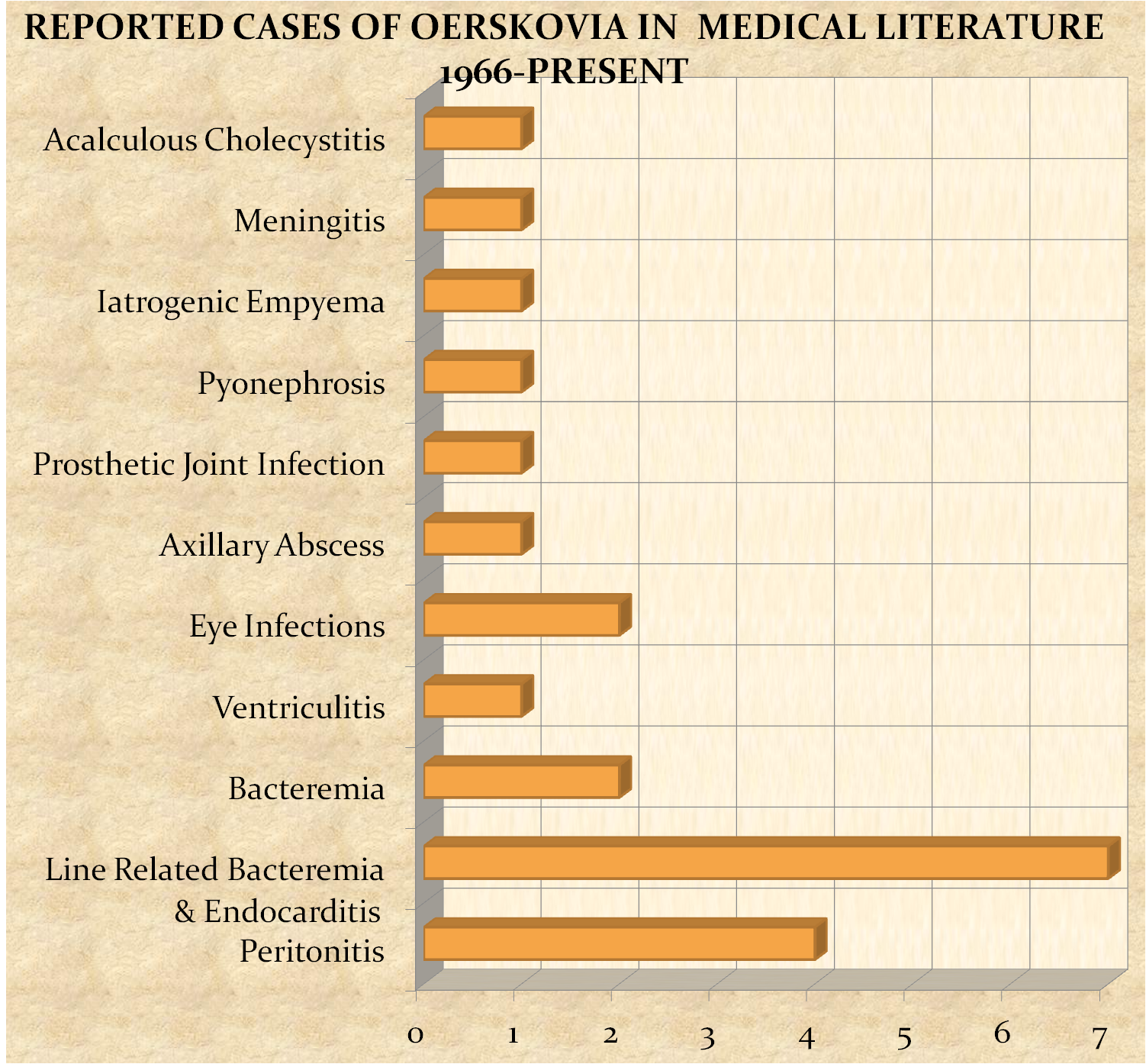
First described by Ørskov in 1938, they are gram positive Nocardia-like bacteria. Often reported as Corynebacterium, a common contaminant, they are found in soil, decaying plant material, sewage and aluminum hydroxide gels. Less than 30 cases have been identified in humans with the majority of cases affecting immunocompromised individuals with foreign body instrumentation. Presentations have ranged from endocarditis, line-related bacteremia, soft tissue infections and peritonitis.
With the upsurge in usage of peripheral lines, catheters and prosthetic material the incidence of Oerskovia may increase in the future with the respiratory tract becoming an important point of inoculation and infection.