Background: Patients are frequently unable to identify their primary hospitalist in the complex hospital environment. Patients may have multiple primary inpatient physicians due to handoffs, may be seen by multiple specialists, and may see housestaff when on a teaching service. This complexity may hinder their ability to identify and engage with their primary attending, and may interfere with the patients’ understanding of their plan of care. This study sought to determine how often patients could identify their primary inpatient physician, and whether correct identification was associated with patients perceiving better understanding of their treatment plan.
Methods: Between January and November 2017, patients who were admitted to a general medicine teaching or non-teaching service were surveyed on hospital day 2 or 3. Patients were asked to identify their main physician during the hospitalization, which was confirmed by chart review. A 4-point Likert scale was used to assess patients’ perceptions of their providers, consultants, the hospital overall, and understanding of their treatment plan. Responses were collapsed into two categories (agree and disagree) for in-text representation and analyzed in the four collected categories (strongly disagree, disagree, agree, and strongly agree) using the Mann-Whitney U test.
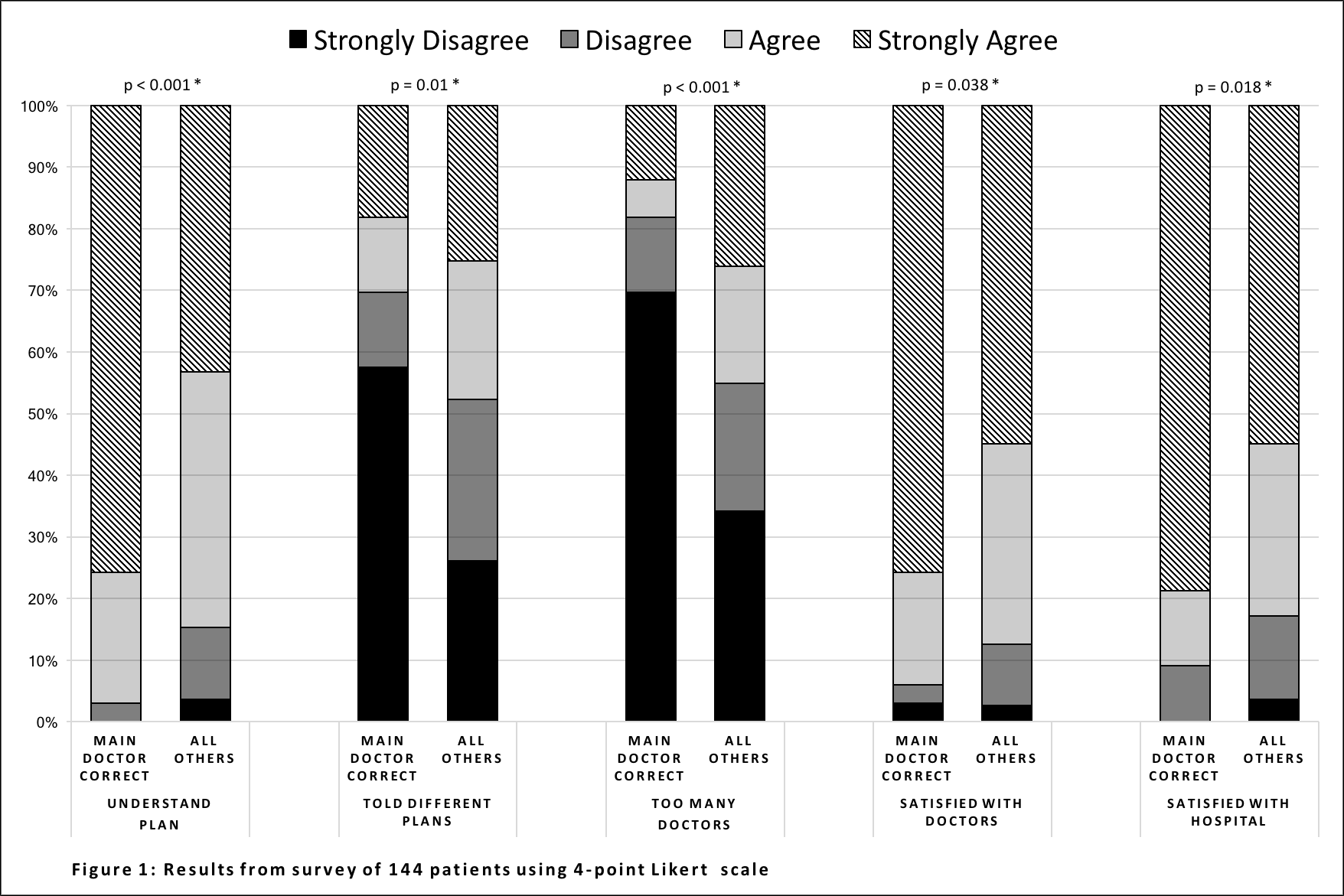
Results: Thirty-three of 144 patients (22.9%) correctly identified (either by name or description) their primary hospitalist, or identified a member of the teaching team as their primary physician. Most patients (89.4%) agreed that knowing their primary provider was important to them, and 77.0% agreed that this would improve their care. Patients who correctly identified their physician were more likely to report understanding their plan of care (97.0% vs 84.7%, p<0.001); less likely to feel as though they had too many physicians involved in their care (18.2% vs 45.0%, p<0.001), and were less likely to feel that they were told different plans of care by different providers (30.3% vs 47.7%, p=0.01). They were also more likely to report satisfaction with their physicians (94.0% vs 87.4%, p=0.04), and with the hospital (90.9% vs 82.9%, p=0.02) (See Figure).
Conclusions: Few patients were able to identify their primary provider or team. However, patients who could identify their provider reported a better understanding of their treatment plan, and identifying their primary provider was associated with increased satisfaction with their physicians and the hospital. While the present study cannot determine whether this relationship is causal, an intervention to improve patient identification of their primary provider might enhance patient satisfaction, engagement, and understanding of their treatment plan.