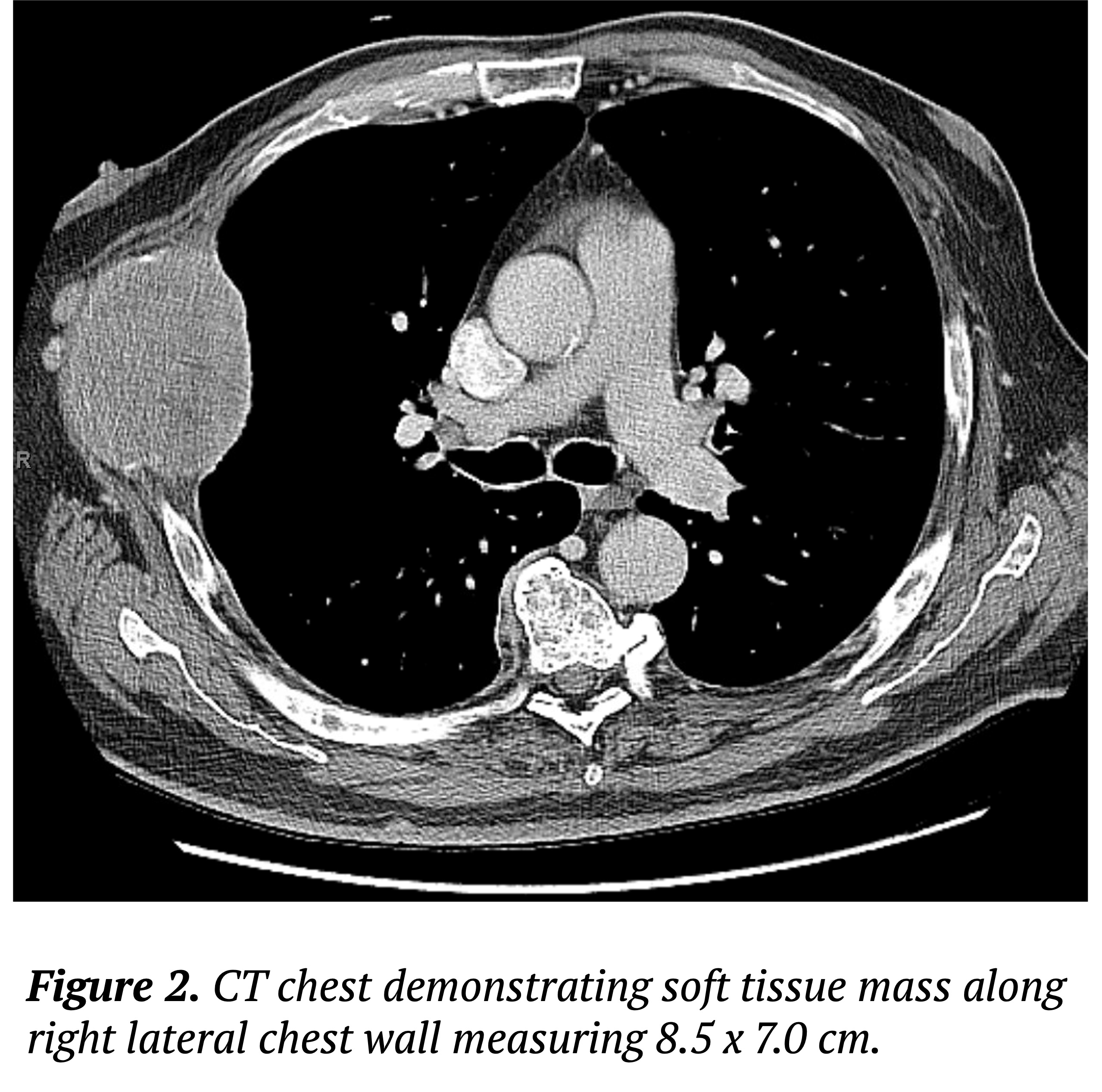
Case Presentation: A 69-year-old male with a history of type 2 diabetes mellitus and hypertension presented with acute-onset encephalopathy in the setting of subacute progressive cough and worsening diffuse pain. Labs revealed corrected calcium 15.1 mg/dl, Hgb 6.8 g/dl, Cr 1.2 mg/dl, total protein 11.9 g/dl, and albumin 2.5 g/dl. Radiological studies showed a large malignant soft tissue mass (8.5 x 7.0 cm) on the right lateral chest wall with satellite lesions and extensive rib destruction suggestive of malignancy of hypercalcemia. The patient’s hypercalcemia improved rapidly with intravenous fluids, diuresis, calcitonin, and bisphosphonate therapy. Despite the resolution of hypercalcemia, encephalopathy persisted. A work-up for multiple myeloma was initiated, revealing IgA 6657 mg/dl, IgG 325 mg/dl, IgM < 20.0 mg/dl, and M-spikes of 3.51 g/dl and 1.03 g/dl on serum protein electrophoresis (SPEP). Alternate differentials for encephalopathy were considered, including HVS. Given the elevated IgA levels, plasmapheresis (PLEX) was initiated. Repeat IgA levels reduced to 3163 mg/dl which was associated with complete resolution of encephalopathy. Blood viscosity level drawn prior to PLEX initiation were elevated at 2.7 rel to H2O, confirming the diagnosis of HVS. Additionally, chest wall mass biopsy and bone marrow biopsy confirmed a plasma cell neoplasm compatible with IgA multiple myeloma. The patient was discharged on a weekly regimen of daratumumab, bortezomib, and dexamethasone. He is currently continuing outpatient chemotherapy, with complete resolution of symptoms.
Discussion: HVS is an oncological emergency that requires prompt therapy to avoid multi-system organ failure. HVS can drive diverse symptomatology at various blood viscosity levels, as the sluggish flow of immunoglobulin-laden blood has the potential to impair the microvascular circulation of many tissues. The most common and reliable symptoms of HVS are oronasal bleeding and visual disturbances according to a variety of studies. This case highlights an unusual case of isolated altered mental status as the presenting feature of HVS. Thus, HVS is an important differential for new-onset encephalopathy in the appropriate clinical context.Another unique feature of this case stems from IgA’s role in developing hyperviscosity. Immunoglobulin driven HVS is typically associated with IgM monoclonal excess due to its pentamer structure, though it can rarely occur with IgA due to its dimeric configuration. Furthermore, it has been demonstrated that IgA levels under 4000 mg/dL are unlikely to lead to clinically significant HVS. Our patient developed symptomatic relief upon decreasing IgA levels to below 4000 mg/dL. Therefore, it is reasonable that lower levels of IgA should dissuade clinicians from pursuing the diagnosis of HVS and subsequently initiating therapy. Treatment of HVS with PLEX is critical to prevent catastrophic multi-organ damage in the short-term, though long-term treatment of the underlying malignancy is required. While blood viscosity levels are helpful in confirming the diagnosis of HVS, testing should not delay initiation of treatment.
Conclusions: Hyperviscosity syndrome can present in settings of significant IgA excess with symptoms of isolated encephalopathy. It is an oncological emergency that requires prompt short-term therapy with plasmapheresis to prevent multi-system organ failure until definitive therapy can be initiated to treat the underlying hematologic condition.