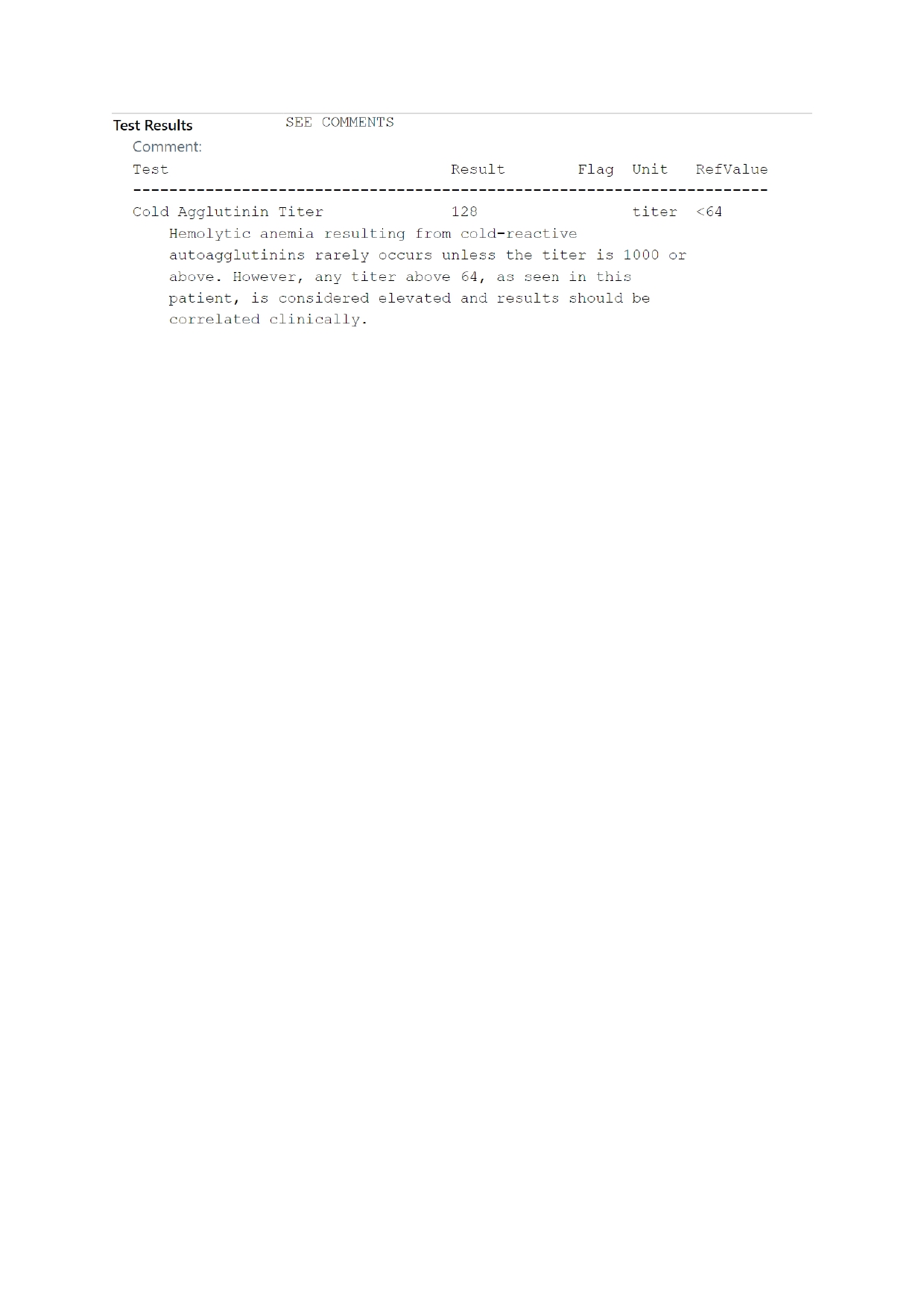
Case Presentation: A 28-year-old man presented with five days of fever, non-productive cough, progressive shortness of breath and hypoxia on admission. CT pulmonary angiography was negative for embolism but revealed multifocal ground-glass infiltrates. Initial management with ceftriaxone and doxycycline for community-acquired pneumonia was started; however, doxycycline was discontinued when atypical infectious workup including respiratory pathogen panel, sputum culture and urinary antigens, returned negative. Despite broad-spectrum antibiotics, his respiratory status worsened over the following week, requiring intubation. On hospital day seven, an unexplained hemoglobin drop from 12 g/dL to 7.9 g/dL without external bleeding prompted hemolysis evaluation. LDH was elevated at 500 U/L (normal < 250); peripheral smear showed RBC agglutination with spherocytes, and direct antiglobulin test was positive, suggesting cold agglutinin hemolysis. Low complement C3 and a cold agglutinin titer of 1:512 confirmed the diagnosis. Bronchoalveolar lavage later detected Mycoplasma pneumoniae. Ceftriaxone was discontinued, doxycycline restarted, and the patient showed rapid improvement with defervescence and successful extubation. This case illustrates how initial negative testing can delay recognition of atypical pathogens. Early identification is essential, as discontinuing targeted therapy or escalating broad-spectrum antibiotics may worsen outcomes. Unexplained anemia with elevated cold agglutinin titers should raise suspicion for M. pneumoniae, even in the absence of confirmatory PCR.
Discussion: Cold agglutinin hemolytic anemia (CAHA) is a rare and often underrecognized complication of Mycoplasma pneumoniae. Immune-mediated hemolysis can significantly alter the disease course, as the resulting anemia worsens tissue hypoxia and mimics progression of pneumonia. Fatigue, tachycardia, and dyspnea from anemia may be misinterpreted as clinical deterioration rather than an extrapulmonary manifestation. Although schistocytes are usually absent, LDH elevation reflects complement-mediated red cell destruction rather than mechanical fragmentation. In CAHA, IgM antibodies bind to erythrocytes in cooler peripheral circulation, activating the complement cascade. The affected red cells undergo hepatic clearance or partial intravascular lysis, releasing LDH. Clinicians should suspect cold agglutinin hemolysis in patients with worsening pneumonia or unexplained anemia, even when early testing for Mycoplasma pneumoniae is negative, as timely recognition and supportive management can prevent hypoxia-related complications and unnecessary blood transfusions, since effective antibiotic therapy often leads to complete resolution.
Conclusions: Negative microbiologic testing does not exclude infection. It is important to maintain a broad differentials in patients with pneumonia and unexplained anemia. Mycoplasma pneumoniae-associated cold agglutinin hemolysis, though rare, should be considered when there is acute onset anemia without an evident source of bleeding in a patient with worsening lung infection. Early recognition, sustained clinical suspicion despite negative tests, and timely initiation of targeted antibiotic therapy are vital to prevent complications and unnecessary interventions. For hospital medicine teams, this case is a reminder that even in an era of algorithmic pneumonia management, the most powerful diagnostic tool remains clinical curiosity.