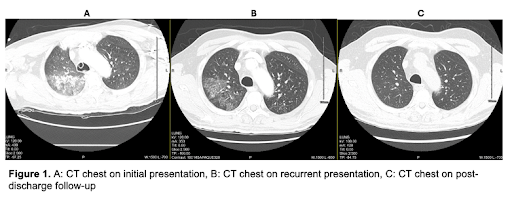
Case Presentation: A 67-year-old man with remote smoking history presented with acute onset hemoptysis and progressive shortness of breath. On presentation, he was tachycardic to 108 bpm, normotensive and hypoxemic to 88% on room air. Physical examination revealed diffuse bilateral crackles without wheezing. Initial laboratory studies showed Hb 9.8 g/dL and normal platelet count and coagulation profile. CRP was 62 mg/L and ESR 20 mm/hr. Blood and sputum cultures, respiratory viral panel, HIV, and Quantiferon were all negative. Autoimmune serologies including ANA, p- and c-ANCA, anti-GBM, rheumatoid factor, anti-CCP, anti-dsDNA, cryoglobulins, and complement levels were unremarkable. Chest X-ray and later CT chest demonstrated bilateral ground-glass and nodular opacities, and bronchoalveolar lavage confirmed diffuse alveolar hemorrhage (DAH). The patient was started on empiric pulse-dose steroids, improved, and was discharged on a steroid taper. Two weeks later, he was readmitted with recurrent hemoptysis. Despite persistently negative serologies, a multidisciplinary team comprising hospital medicine, pulmonary, rheumatology, interventional radiology, and critical care suspected isolated pauci-immune pulmonary capillaritis (IPIPC). Cyclophosphamide was recommended, but after shared decision making, IV rituximab was administered instead due to side effect profile, resulting in symptom resolution.He was readmitted a third time two weeks later for massive hemoptysis. Repeat bronchoscopy and endobronchial biopsy ruled out infection and malignancy but were otherwise non-diagnostic. Following stabilization with corticosteroids, he received a second rituximab infusion and began a slow prednisone taper. Over the subsequent six months, he remained clinically stable with no further bleeding episodes. He continues regular outpatient follow-up with pulmonology and rheumatology, receiving scheduled rituximab maintenance infusions without recurrence.
Discussion: Diffuse alveolar hemorrhage carries up to 50% mortality when diagnosis is delayed. Seronegative or IPIPC is rare but increasingly recognized, and up to 20% of ANCA-associated vasculitides may initially be seronegative. This case highlights the hospitalist’s role in maintaining diagnostic persistence, re-evaluating prior assumptions, and pursuing empiric therapy when the clinical picture suggests immune-mediated disease despite unrevealing serologies.Empiric corticosteroids remain first-line therapy, while rituximab offers effective induction and maintenance with fewer cytopenic and oncologic risks than cyclophosphamide. Beyond therapeutics, this case underscores the importance of resisting premature diagnostic closure and maintaining an open differential when the etiology remains uncertain. Coordination between inpatient and outpatient teams was critical to ensure immunotherapy completion and durable remission.
Conclusions: Seronegative autoimmune lung disease challenges data-driven reasoning and highlights the importance of persistence and pattern recognition in hospital medicine. Hospitalists must balance evidence with clinical intuition, maintain vigilance for immune-mediated disease even in the absence of serologic confirmation, and ensure collaboration across disciplines. Sustained remission on maintenance rituximab underscores the impact of continuity and multidisciplinary care in complex diagnostic scenarios.