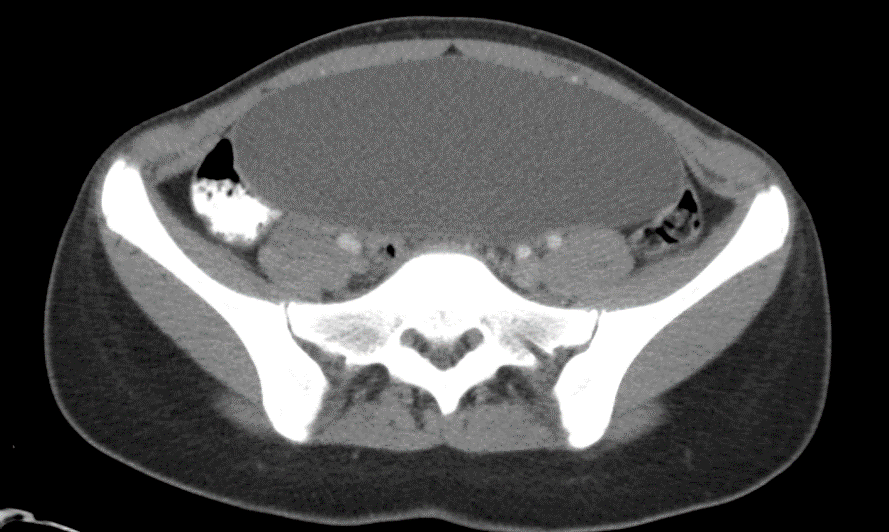
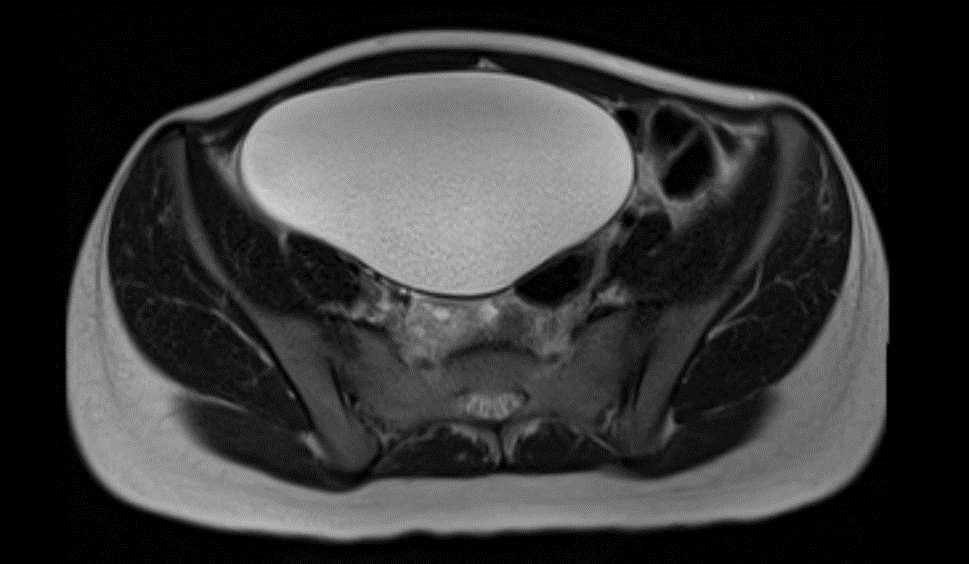
Case Presentation: A 15-year-old female was referred to the hospital by her urologist for persisting urinary retention and bladder distention concern. The patient endorsed 5 months of increased urgency and decreased frequency of urination, as well as a decreased amount during each void. She denied dysuria, gross hematuria, incontinence, or history of UTI. She had not experienced fever, nausea, constipation, diarrhea, or abdominal pain. Her grandparents had hypertension, type 2 diabetes, and hyperlipidemia, in addition to lung, colon, and bladder cancer. On physical exam there was notable firm, mid-lower abdominal distention. There was no guarding, tenderness with palpation, or organomegaly. Prior abdominal and pelvic ultrasound, urodynamic testing, cystoscopy, and bilateral retrograde pyelogram results were all normal.A CT of the abdomen/pelvis revealed a large, simple fluid-filled cystic mass at the midline. A subsequent MRI showed a 17.3 x 15 x 8.6 cm unilocular cyst appearing to arise from the right adnexa. The size was concerning for malignancy, so serum tumor markers were obtained of alpha-fetoprotein (1.1 ng/mL), lactate dehydrogenase (136 U/L), and beta human chorionic gonadotropin (negative) – all in normal range. Differential diagnoses at this point included urachal cyst, serous cystadenoma, simple ovarian cyst, or paraovarian cyst. Ovarian cancer was also possible given family history of other cancers. After surgical excision, pathology results confirmed a benign right ovarian serous cystadenoma.
Discussion: Ovarian cysts are found commonly in women of various ages but are far less typical in children and adolescents. This patient’s presentation was unique since ovarian tumors in pediatric patients usually present with some abdominal/pelvic pain or discomfort. Although a lower abdominal mass was seen and palpated on physical exam, the patient’s ongoing symptoms of urinary retention, increased urgency, and decreased void initially suggested a bladder distention or obstruction rather than an ovarian tumor.Most ovarian cysts in the pediatric population are characterized as physiologic, while comparatively fewer are found to be neoplastic. Neoplastic tumors require more extensive management with consideration of possible ovarian torsion, malignancy, and surgical intervention. If there is concern for malignancy, as indicated with our patient’s large tumor size and family history, hospitalists may collect a panel of serum tumor markers. Key markers include beta-hCG, AFP, CA 125, LDH, Inhibin A, and Inhibin B. Although they vary in sensitivity and specificity, elevations can be seen with malignant tumors. Treatment options for pediatric ovarian cysts range from watchful waiting to prompt surgical intervention. The decision depends on tumor size, patient age, severity of symptoms, and possibility of acute and long-term complications. If a lesion is significantly large (> 8-10 cm), surgical removal is preferred due to reduced likelihood of spontaneous resolution and increased risk of torsion and malignancy. Surgical excision of large ovarian tumors has a risk of rupture or secondary surgery. However, laparoscopic ovarian cystectomy with fertility-sparing techniques is recognized as safe and effective for patients with large, benign cystadenomas.
Conclusions: Benign serous cystadenomas of the ovary are rarely seen in pediatric patients. When faced with exclusively urinary symptoms and ambiguous initial imaging, pediatric hospitalists should consider a gynecologic diagnosis.