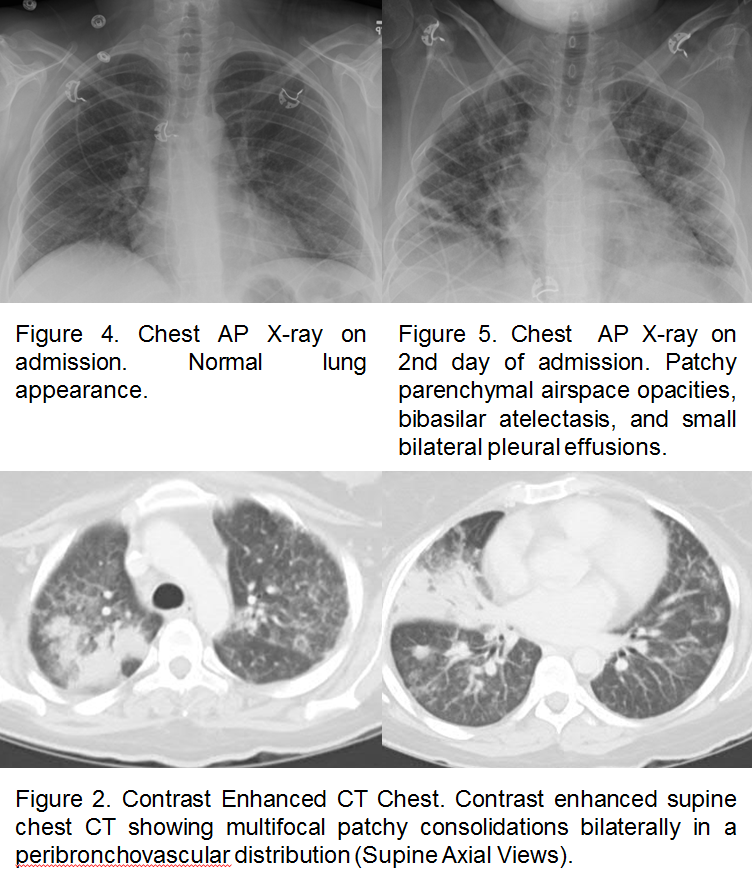
Case Presentation: A 32-year-old woman with history of lupus not on steroid or immunosuppressive therapy for more than 10 years presented with headache, generalized weakness, abdominal pain, nausea, vomiting, and malaise. On exam, the patient was afebrile with tachycardia and hypotension. She was ill-appearing with a diffusely tender abdomen, mild hepatomegaly, and enlarged axillary and inguinal lymph nodes. Neurologic and pulmonary examination was normal. Laboratory evaluation was significant for a white blood cell count of 49 x 10^9/L with 55.4% atypical lymphocytes, elevated liver enzymes and positive ds-DNA antibodies. Plain film of the chest was unremarkable, and computed tomography of the abdomen showed hepatosplenomegaly and diffuse lymphadenopathy. The patient was admitted with the diagnosis of sepsis and treated with fluids and antibiotics. On the day of admission, the patient developed confusion and blurring of vision. An extensive work up including brain magnetic resonance imaging, ophthalmologic examination, and lumbar puncture were negative. Lymph node biopsy and flow cytometry were negative for hematologic malignancy. Cytomegalovirus IgG and IgM serology was positive with a viral load of 9,140 by cytomegalovirus DNA polymerase chain reaction. The patient remained afebrile during admission developed hypoxic respiratory failure and required intubation. Chest imaging showed multifocal patchy infiltration bilaterally. Bronchoscopy sampling was positive for cytomegalovirus. She was treated with ganciclovir with significant improvement and complete recovery on follow up visit.
Discussion: Cytomegalovirus infection in immunocompetent hosts is common but usually asymptomatic and self-limited not requiring hospitalization. Severe and tissue invasive infection/reactivation requiring hospitalization are seen in patients with impaired cell-mediated immunity such as in acquired immunodeficiency syndrome (AIDS), transplant patients, or patients on immunosuppressive therapy including steroids. T cells play a vital role in CMV virus replication and controlling disease. An effective immune response to CMV is required otherwise viral replication and immune evasion leads to dissemination and tissue invasion as seen in this case.
In the absence of immunomodulating therapy, patients with autoimmune diseases, such as our patient with untreated lupus, are not typically regarded as immunocompromised hosts. However, there is mounting evidence that suggests that immune dysregulation in lupus increases susceptibility to unusual and severe viral infections. Timely recognition and treatment by hospitalists is necessary to reduce morbidity and mortality.
Conclusions: This is a rare case of tissue invasive cytomegalovirus infection in an immunocompetent patient, and hospitalists should maintain a higher index of suspicion for atypical infections in patients with lupus even if they are not immunosuppressed.