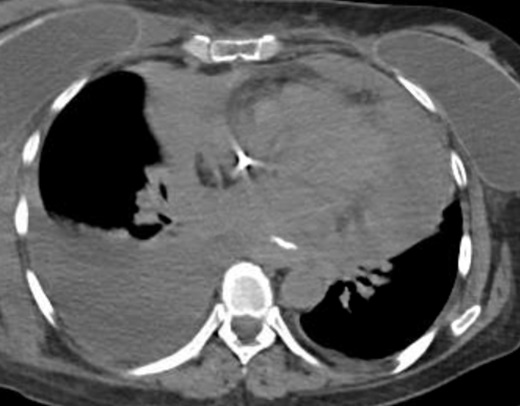
Case Presentation: This is the case of a 57-year-old lady with rapidly progressive stage IV pulmonary adenocarcinoma who presented two months after diagnosis with findings of significant hyponatremia. Upon admission, she was afebrile, hypotensive and tachycardic. Sodium was 119 mEq/L, potassium 2.4 mEq/L, chloride 67 mEq/L, serum osmolality 246 mosm/kg, urine osmolality 684 mosm/kg and urine sodium 41 mEq/L. Her presentation was consistent with Syndrome of Inappropriate Antidiuretic Hormone, but her hyponatremia did not improve despite adequate management with fluid restriction and salt tabs. During hospitalization, she was also found to have a large pericardial effusion with echocardiographic evidence consistent with tamponade physiology that required an emergent pericardial window. Following pericardial drainage, her hyponatremia improved to 128 mEq/L and continued to uptrend, suggesting a correlation between her hyponatremia and malignant pericardial effusion leading to cardiac tamponade.
Discussion: A handful of published reports present a similar scenario in which pericardial drainage resulted in immediate resolution of the hyponatremia, particularly in patients with underlying malignancies. It is suggested that a decreased cardiac output stimulates antidiuretic hormone release and suppresses atrial natriuretic factor release, causing volume retention, an adrenergic increase in heart rate and increased peripheral resistance. Following pericardiocentesis, there is marked diuresis and a normalization in sodium concentration. Two retrospective studies (Bor-Hsin, 2016; Chang, 2012) evaluated the incidence of hyponatremia in patients with cardiac tamponade of malignancy and non-malignancy related etiologies. They found that patients with malignancy-related tamponade had higher rates of hyponatremia and a more significant improvement in the sodium levels following pericardial fluid drainage. However, the incidence and underlying mechanism of this presentation remain unknown.
Conclusions: Cardiac tamponade should be included in the differential of hyponatremia in patients with active malignancy since prompt management with pericardial drainage can result in marked improvement of hyponatremia.