Background: At academic institutions and other referral centers the process of accepting transfers from other hospitals has been a challenging and potentially laborious process to coordinate smoothly. It was also one that was not previously reimbursable. However, beginning in 2017 Medicare and other insurance companies began reimbursing Non-Face-to-Face Prolonged services procedural codes. These new codes allowed providers to bill for time spent reviewing records and coordinating care with other physicians either before or after a patient encounter if the total time spent doing this was at least 30 minutes.
Purpose: To use these new Non Face-to-Face prolonged services codes to be reimbursed for the time spent accepting some of the transfers from other hospitals when that work was documented in the medical record.
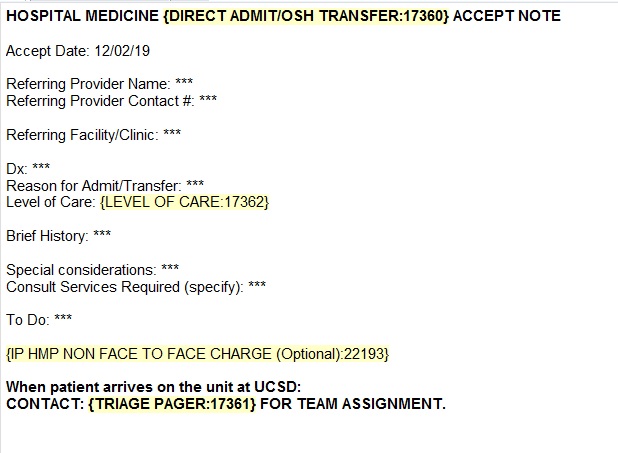
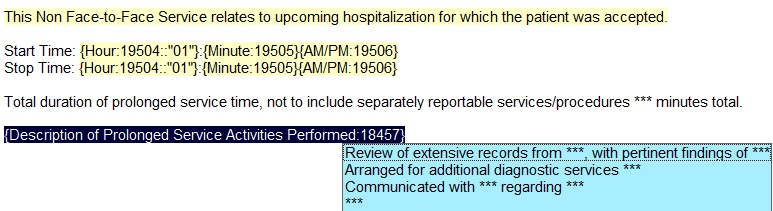
Description: At our institution accepting transfers from other hospitals involves communication with a transfer center to find out the gist of the transfer request and to determine who at the other facility to call. Then, the hospitalist briefly reviews any records about the patient already available in our electronic medical record. They then call the requesting physician to gather pertinent information about the patient’s stay at the other facility. If the reason for transfer is a procedure, many times the hospitalist also will contact the proceduralist to see if the request is reasonable. Finally, after the hospitalist has informed the requesting physician that they are willing to accept the transfer request, the hospitalist then completes an outside hospital transfer accept note in the hospital encounter that was created by the transfer center. This note briefly summarizes all of the previous conversations to allow the hospital medicine team that is on-call when the accepted patient arrives to quickly understand the patient’s course at the sending hospital, the reason for transfer, and the first steps to take when the patient arrives.After discussions with our institution’s billing and compliance office. We had the CPT codes for Non-Face-to-Face Prolonged Service charges (99358 and 99359) added to the ones we could submit from within an inpatient encounter. We then added an optional section to our outside hospital accepted transfer note template that included the required language for the Non-Face-to-Face prolonged service code to use when accepting a transfer took longer than 30 minutes and educated our hospitalists about how to use this new code.We obtained data on the number of Non-Face-to-Face Prolonged Services charges that our hospitalist submitted in the first 12 months of use and the number of those submitted charges that were paid. We collected on 80.3% of the Non-Face-to-Face Charges we submitted for an average return per charge paid of $95.33 and an average return per charge submitted of $75.25. The collection rate on the charges for the division of hospital medicine was roughly the same as the institution as a whole (81%) with the vast majority of the other claims coming from the outpatient setting.
Conclusions: Thus, for little extra work above what we were already doing in accepting transfers from other hospitals, hospitalists at our institution were able to submit Non-Face-to-Face prolonged service charges and get paid for their work. Our approach to generating this net new revenue stream utilizing the notes that we already use in accepting patients in transfer from other hospitals may be useful to other hospital medicine groups who have similar opportunities to capitalize on this workflow.