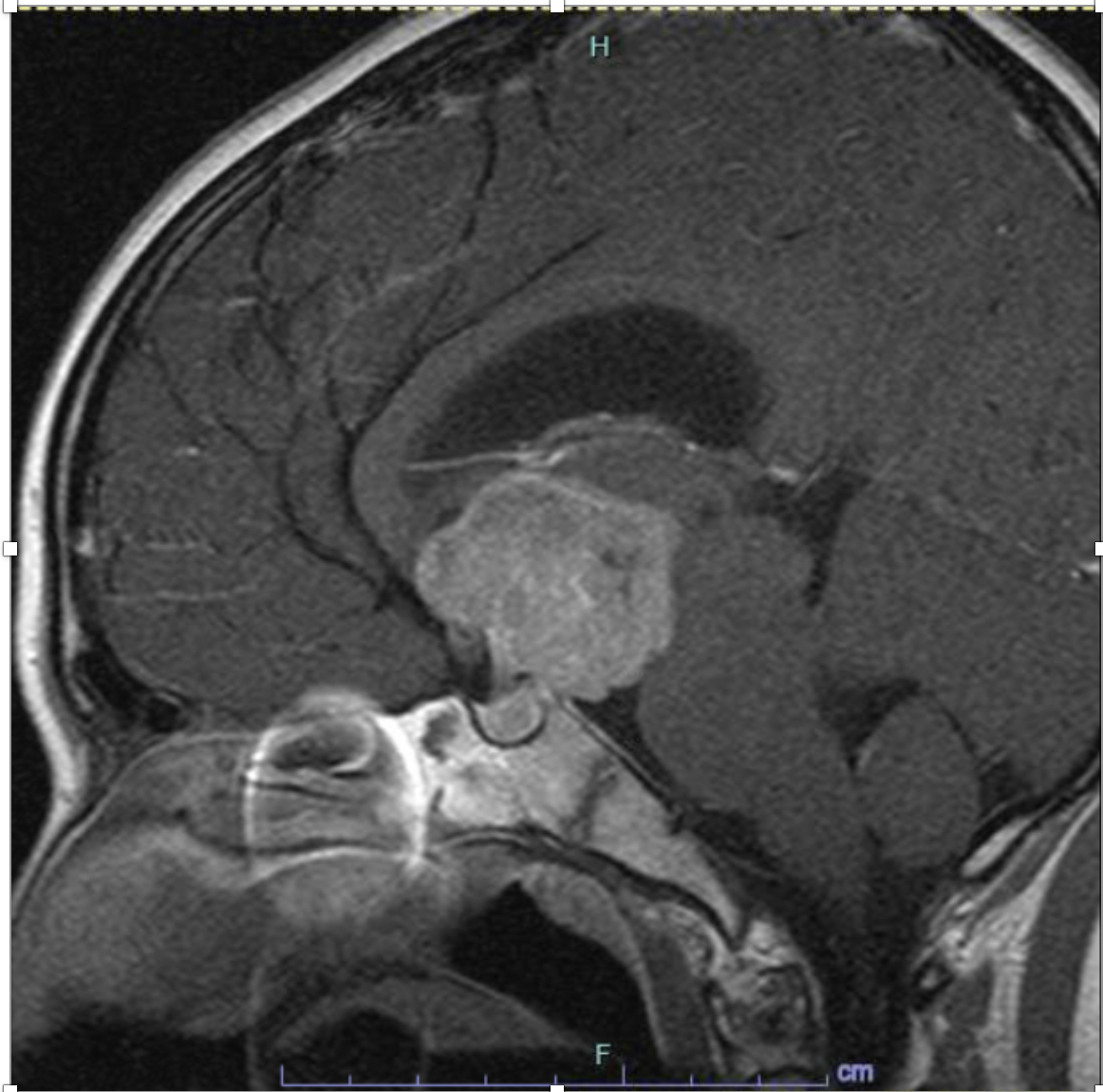
Case Presentation: 14-year-old female with history of depression, anxiety, and sexual abuse was referred to the adolescent clinic with 4 months of rapid weight loss, vomiting, and occasional headaches. Further history revealed several months of hiding and refusing food, although she denied body dysmorphia. Her exam revealed a pre-pubertal female with absent secondary sex characteristics, normal neurologic exam and positive orthostatic vitals. She was admitted for severe malnutrition secondary to possible anorexia nervosa and started on an eating disorder protocol. Lab work on admission was significant for undetectable LH, FSH, estradiol and TSH levels, normal T3 and T4, elevated ESR to 30 and negative celiac screen. During admission, she refused all oral nutrition and nasogastric feeds were initiated. She then developed polyuria, hypernatremia, hyperchloremia and hypoosmolar urine consistent with diabetes insipidus. Additional labs revealed a morning cortisol of 1ug/dL and prolactin of 103.2ng/mL. MRI of the brain revealed a large suprasellar mass with moderate hydrocephalus and significant compression of the pituitary gland. Her symptoms were suggestive of panhypopituitarism secondary to mass effect. Her symptoms improved with desmopressin and hydrocortisone replacement. She was then transferred to another center for neurosurgical evaluation and underwent transsphenoidal biopsy, which revealed a germinoma. Chemotherapy was started with plans for future radiation treatment.
Discussion: Germinomas are a form of intracranial germ cell tumor, which comprise 3-15% of primary pediatric intracranial neoplasms. Most cases are diagnosed in patients less than 20 years of age with peak incidence between 10-12 years old. Males are more commonly affected than females. Location vary by sex, with suprasellar location being more common in females, as in our patient, and pineal locations being more common in males. Diabetes insipidus is the most common endocrine manifestation and can precede radiologic diagnosis. Other endocrine abnormalities such as delayed or precocious puberty, growth retardation, and hypopituitarism can also be seen (1).
Conclusions: In a patient with a history of trauma and restricted food intake, cognitive biases such as anchoring and framing can lead to premature closure. This patient’s history was initially concerning for anorexia nervosa, however she failed to meet diagnostic criteria and lacked body dysmorphia. While there are known hormonal changes associated with anorexia, her suppressed TSH, undetectable gonadotropins, low cortisol and elevated ESR were inconsistent with typical findings(2,3). In addition, fluid restriction as part of her structured eating disorder protocol proved to be problematic in this patient. Because she could no longer compensate for her underlying diabetes inspidus with unrestricted fluid intake, this contributed to the rapid development of hypernatremia. This case highlights the dangers of premature closure, which could have led to continuation of inappropriate therapy with delay in correct diagnosis and treatment in a patient with a much more sinister diagnosis. She is currently undergoing chemotherapy with plans for future radiation treatment.