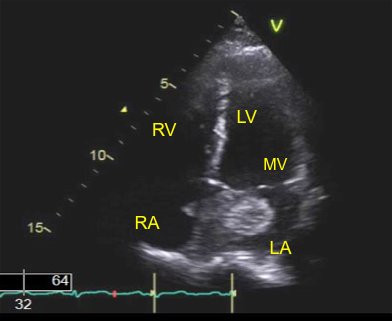
Case Presentation: This is a 49 year old female, with no significant medical history, who started having intermittent fevers, night sweats, and fatigue 11 months prior. She reported a temperature of 100.4°F with cough and rhinorrhea, diagnosed as bronchitis with an elevated CRP of 40 mg/L. She reported some improvement with azithromycin but continued to have worsening fatigue and 2 months later, she was admitted for vertigo and presyncope. Her NIH stroke scale score was 0 and CT scan of her brain was negative for acute pathology. She was diagnosed with peripheral vertigo. She continued to have fatigue and reported 10 pound weight loss over a period of 6 weeks. Her CRP continued to be elevated to 140 mg/L, prompting an infectious disease workup which was inconclusive. She was then referred to Pulmonology but due to complaints of chest pain described as substernal, 4/10 pressure, she was referred to Cardiology. Physical exam was significant for a 1/6 holosystolic murmur at the left sternal border. Electrocardiogram showed normal sinus rhythm with no ischemic changes. Transthoracic echocardiogram showed left ventricular ejection fraction of 55-60% and a mass in the left atrium estimated as 2.8 x 3.4 cm (Figure 1). Cardiothoracic Surgery was consulted for myxoma and the patient agreed to surgical resection via sternotomy. The gross specimen measured 6.2 x 4.3 x 2.9 cm (Figure 2). Histological evaluation of the specimen showed mostly matrix composed of an acid-mucopolysaccharide-rich stroma consistent with a myxoma but negative for malignancy.
Discussion: This patient’s intermittent fevers were likely due to associated inflammatory cytokines such as interleukin-6 and other acute phase reactants such as CRP. This patient’s episode of vertigo and presyncope may have been a transient ischemic attack associated with micro emboli from the myxoma. Given the rarity of sporadic myxoma, 0.5 per million population per year, the syndrome of Carney complex (CNC) is of interest whereby myxomas are seen in about 30%–60% of cases and the recurrence rate can be as high as 21%. Carney complex is an autosomal dominant multiple neoplasia syndrome linked to the PRKAR1A gene on chromosome 17q22-24 that includes cardiac myxoma, familial multiple endocrine neoplasia syndrome and pituitary somatomammotrophic adenomas. Extra-cardiac manifestations include pigmented skin lesions, cutaneous myxomas, adrenal cortical disease, myxoid mammary fibroadenoma, and testicular tumors. Although the patient was not diagnosed with CNC, genetic counseling may be beneficial if her myxoma recurs.
Conclusions: Clinical features of myxomas encompass a triad of arterial embolism, obstruction of intracardiac blood flow, and constitutional signs. This array of symptoms poses a diagnostic challenge as the differential diagnosis can include rheumatic mitral valve disease, pulmonary hypertension, endocarditis, myocarditis and vasculitis. However, if a cardiac myxoma is suspected, echocardiography should be performed with subsequent cardiothoracic surgical evaluation due to the risk of sudden cardiac death associated with mitral valve obstruction and 35% risk of embolization leading to stroke. Although surgical resection is curative and recurrence rate is low, about 5%, patients may benefit from serial echocardiograms. It may be interesting to follow patients with CNC and myxoma as this larger sample size may provide data to optimize presurgical management in minimizing embolic complications and sudden cardiac death.