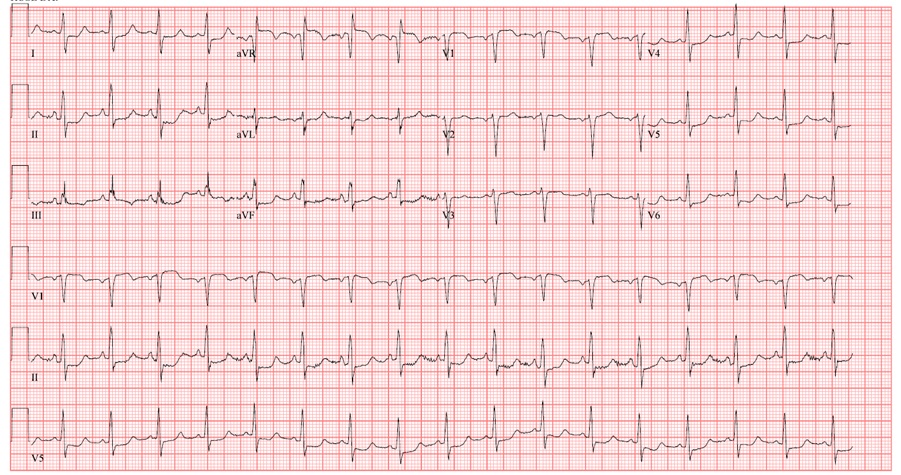
Case Presentation: A 49-year-old female with history of hypertension, obesity, depression and intermittent cocaine use presented to the emergency department with a syncopal episode while at the grocery store. On arrival she was hypotensive to 80/58 with a new 4-liter oxygen requirement. Electrocardiogram (ECG) showed ST elevations in leads aVR and V1 with ST depressions in II, III, aVF as well as V4 through V6. CT angiogram was performed and revealed acute saddle pulmonary embolus (PE) with echocardiogram showing left ventricular ejection fraction of 50 percent and both right atrial and ventricular dilation. ECG changes and respiratory failure improved with fluid resuscitation, and the decision was made not to pursue thrombolytic therapy. She was started on a heparin drip, transitioned to apixaban, and discharged. However, she was re-hospitalized at our facility three days later with elevated troponin, persistent T-wave inversion with concern for ischemia, worsening PE or cocaine-induced vasospasm. In a following hospitalization, cardiac catheterization was pursued with no angiographic coronary artery disease identified.
Discussion: The electrocardiographic pattern of ST elevations in leads aVR and V1 with concomitant ST depressions in acute PE has been previously described, but is not well known to the hospitalist community. This pattern has been shown to correlate with hemodynamic instability and higher complication rates in patients with acute PE. In patients with this ECG pattern who undergo coronary angiography due to concern for acute ST elevation myocardial infarction (STEMI), acute coronary occlusion is rarely encountered..
Conclusions: This case highlights the importance of recognizing the ECG pattern of ST elevations in leads aVR and V1 for any provider triaging acute PE. It is rarely a sign of acute coronary occlusion, and can serve as a potential marker to predict hemodynamic instability and potential need for a higher level of care. Recognizing this pattern has the potential to risk stratify patients with acute PE and prevent unnecessary procedures.