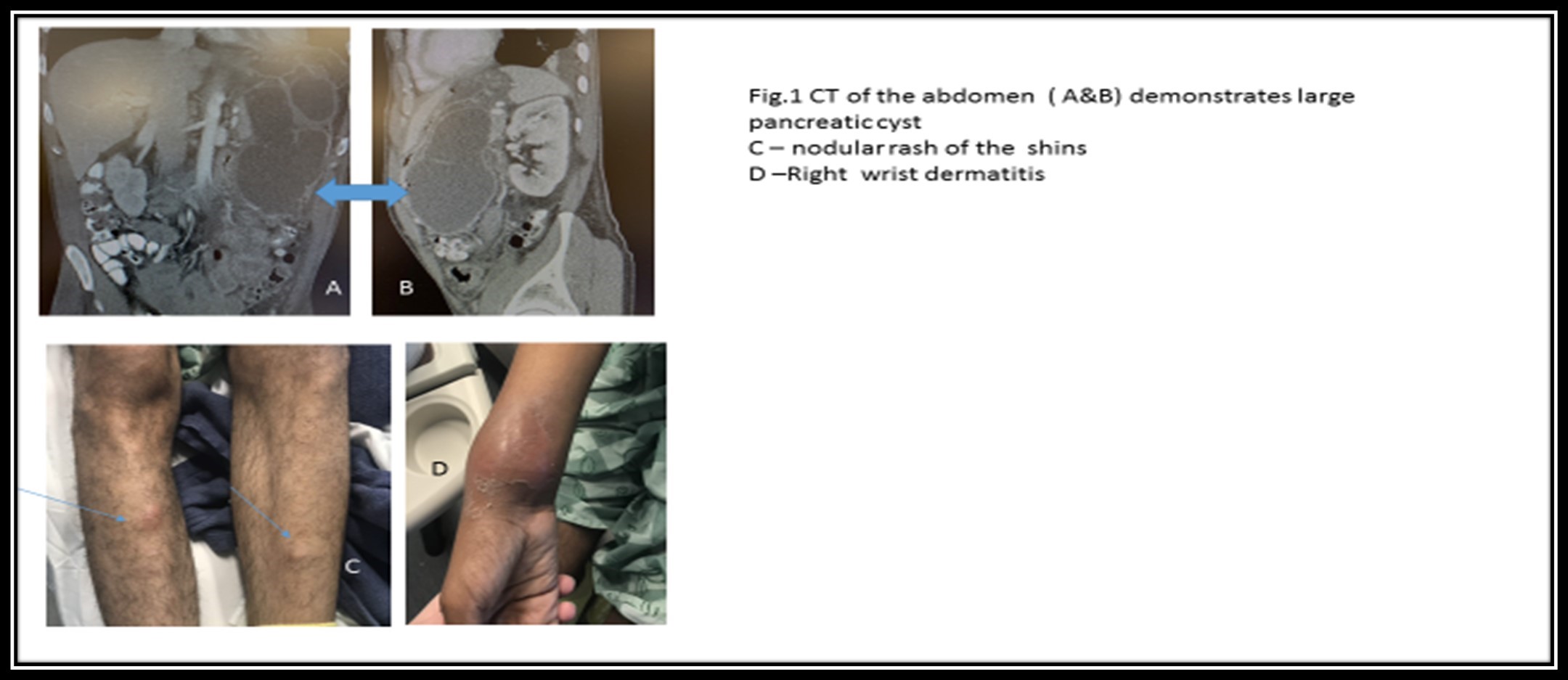
Case Presentation: A 41- years- old male with no medical problems but daily alcohol and tobacco abuse developed sudden right and then left foot pain with swelling 2 weeks before admission. Diagnosis of gout was diagnosed at another hospital and he was treated with steroids with no symptom relief; the right wrist swelling prompted empiric antibiotic administration for concern of infection, radiological studies including multiple joint XRs, MRI, and a Doppler studies were un-revealing. Due to ongoing fever and polyarticular pain including the right distal forearm, both ankles, multiple PIP joints, he was admitted to our hospital. Laboratory data detected leukocytosis, increased inflammatory markers, synovial fluid from the left ankle yielded brownish-yellow viscous thick material with non-inflammatory features, and sterile culture. During the hospitalization, abdominal discomfort developed, which prompted us further evaluation: lipase was elevated up to 945 mcg/dL (80 mcg/dL reference) and abdomen images demonstrated pancreatic parenchymal calcifications and a large multiloculated cystic structure concerning chronic or acute pancreatitis (Fig.1 A&B). During the hospitalization he developed a nodular rash of the shins (fig.1. C), skin biopsy detected lobular panniculitis with ghost cells confirming the presence of pancreatitis panniculitis and PPP syndrome. Due to the large size of the pancreatic cyst resection was not advised. He was discharged home with empiric antibiotics for possible right wrist osteomyelitis, a prednisone taper, and a recommendation to stop alcohol. Six months later he is off steroids, feeling much better, works, and lives independently.
Discussion: An uncommon syndrome of lobular panniculitis, pancreatitis, and polyarthritis (PPP) syndrome is a form of subcutaneous fat necrosis, multiple joint arthritis associated with underlying pancreatic disease. It is hypothesized that pancreatic enzymes release to the bloodstream leading to systemic lipolysis and fat tissue necrosis of subcutaneous tissue and bone marrow. Here we report a case of PPP-syndrome with pancreatitis associated with extensive panniculitis and diffuse polyarthritis.
Conclusions: ConclusionDiagnosis of PPP syndrome is challenging since abdominal symptoms may be lack or mild. Without specific treatment of underlying pancreatitis, the prognosis of this condition is poor. The common complication is chronic arthritis with a poor response to nonsteroidal anti-inflammatory drugs and corticosteroids.