Background: The clinical evaluation of febrile infants less than 28 days has been extensively studied with the aim to improve the sensitivity in identifying those infants at risk for invasive bacterial infections while decreasing the harm of unnecessary invasive diagnostic procedures. Even though bacterial meningitis is associated with high morbidity and mortality, the incidence is low. In 2018, our institution implemented a clinical pathway for febrile infants 7-28 days utilizing a new risk stratification protocol limiting lumbar punctures (LP) in those classified as low risk. The objective of this study is to evaluate the number of safely avoided LPs and the incidence of missed cases of meningitis.
Methods: We performed a retrospective study of full-term infants aged 7-28 days who presented to the emergency department (ED) between 2018-2022 for fever and managed on the febrile infant clinical pathway. Patients were identified utilizing ICD-10 codes for fever, bacteremia, urinary tract infection (UTI), pyelonephritis, and meningitis and all charts were manually reviewed. Data collected included demographics, bacterial cultures results, and LP procedures. Infants who presented as ill-appearing, with signs of focal infection, or with seizure were excluded. Per the pathway, infants were classified as low-risk if they did not have any of the following criteria: history of prolonged hospitalization, prolonged newborn nursery course or history of unexplained hyperbilirubinemia, complete blood cell count (CBC) with white blood cell count (WBC) < 5000/cc or >15000/cc or >1500/cc bands, positive urinalysis (UA) for nitrites, leukocyte esterase or WBC >5/HPF, procalcitonin >1 ng/ml. If an infant met criteria for low-risk, only CBC, procalcitonin, blood culture, UA, and urine cultures were recommended but LP and antibiotics were not required. Descriptive statistical analysis was used to analyze the data.
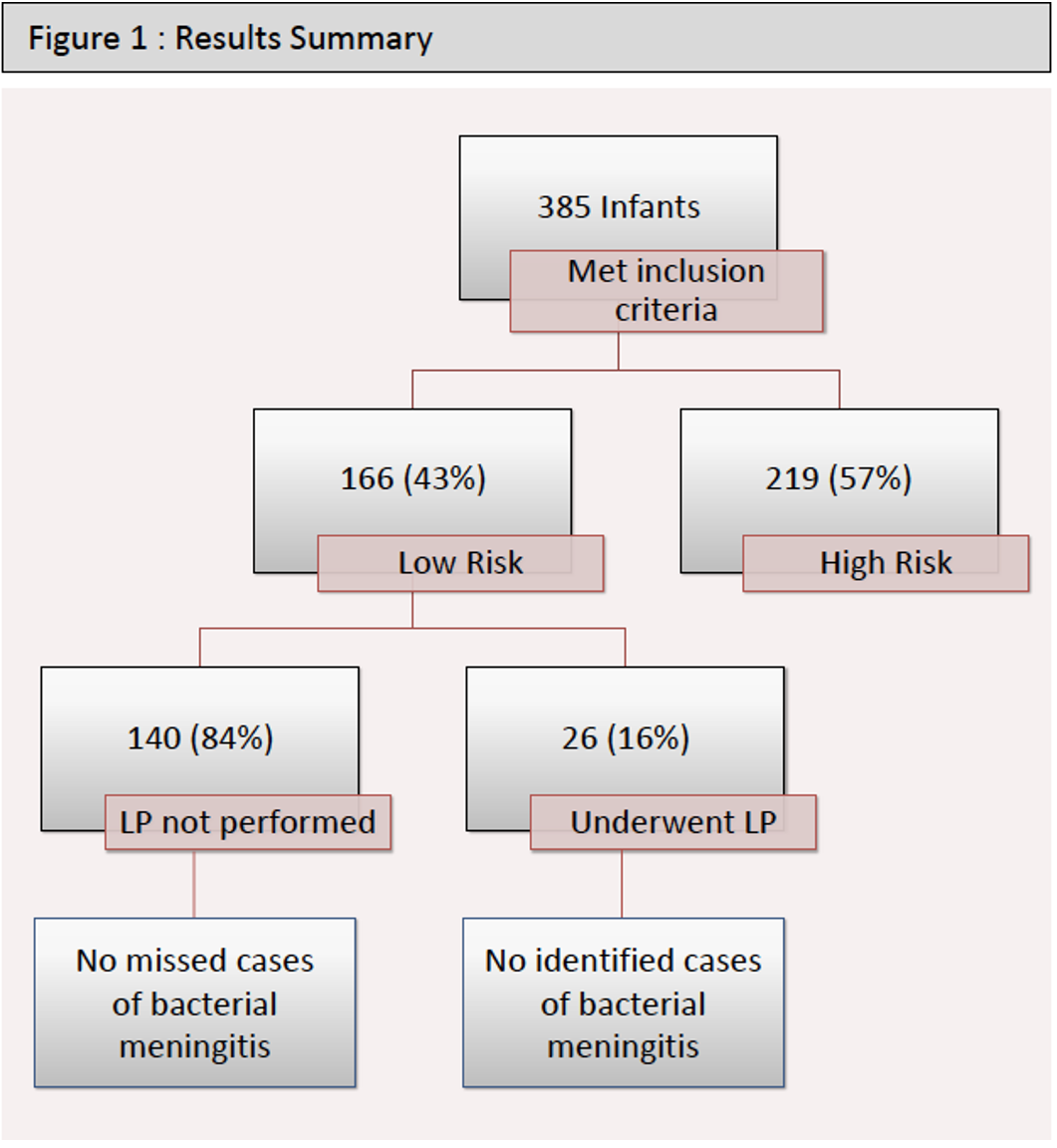
Results: 385 infants met inclusion criteria; 166 (43%) were classified as low-risk and 219 (57%) were high-risk. Mean age of the low-risk group was 19.5 days. Of the 166 low-risk infants, 140 did not undergo LPs per the clinical pathway. However, 26 infants who met low risk criteria per the clinical pathway did undergo a LP: 13 had LPs performed at an outside hospital prior to transfer to our ED; 7 were done based on the ED clinicians’ judgment; 4 were performed after admission due to positive blood and/or urine cultures; 1 performed for increasing fussiness; and 1 for development of seizures after admission. Of the 140 low-risk infants that did not undergo a LP, there were no cases of missed meningitis. Of those who had a LP performed, none were found to have bacterial meningitis, but one case of viral meningitis was detected.
Conclusions: Based on our study, lumbar punctures can be safely avoided in low-risk febrile infants 7-28 days without any cases of missed bacterial meningitis.