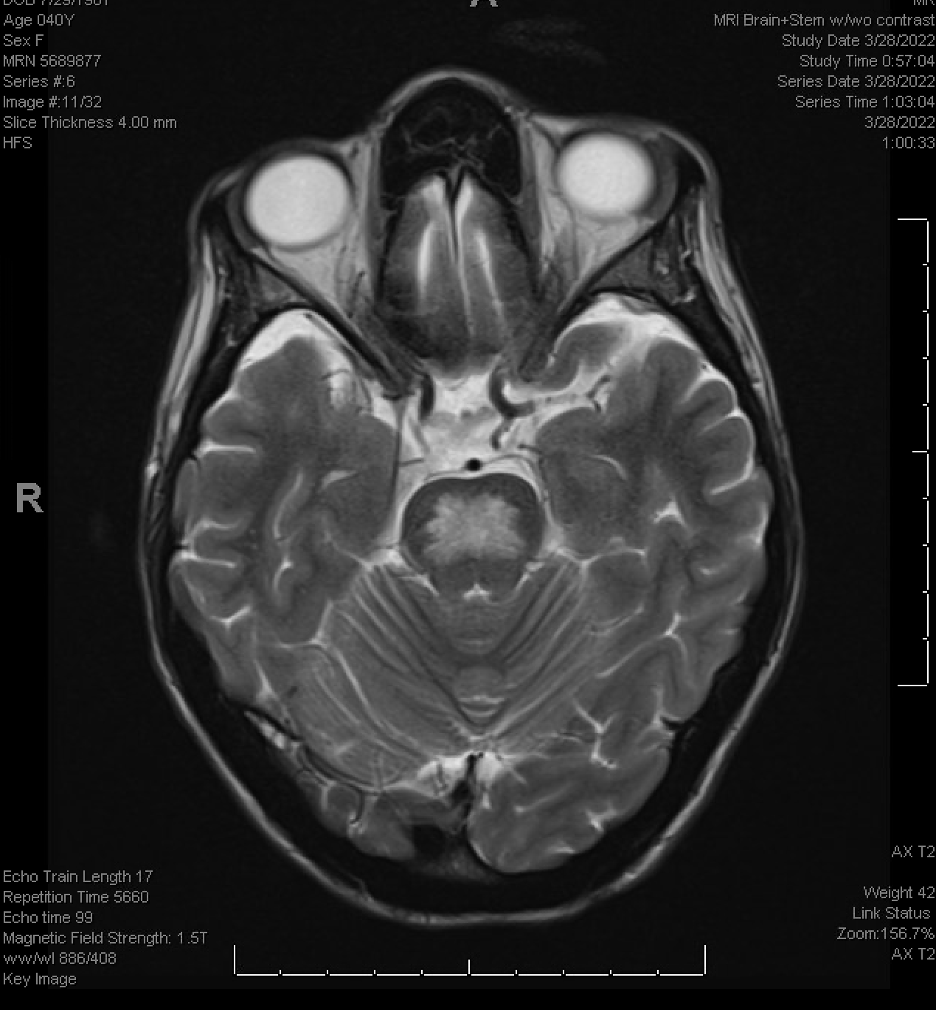
Case Presentation: A 40-year-old woman with diabetes mellitus type 2 and severe malnutrition presented to our institution with symptoms of altered mental status and dysuria. Initial evaluation was most notable for a capillary blood glucose of 1113 mg/dL and initial sodium of 125 mEq/L (which corrected for glucose level was within the normal range of 141-149 mEq/L). She was diagnosed with HHS and treated with IV fluids and insulin. Throughout the course of the hospitalization, the patient developed progressive bilateral lower extremity weakness, subacute severe urinary retention, bowel incontinence, and flaccid rectal tone. Additionally, she experienced progressive dysphagia and trouble swallowing throughout the admission. Upon further questioning, she stated that weakness began when she came to the hospital. An MRI brain was obtained which showed T2 hyperintensity of the pons suggestive of ODS (Figure 1). Other diagnoses were ruled out such as stroke, multiple sclerosis, and hypertensive encephalopathy. The patient improved later in her hospital course and was treated supportively. She was evaluated by PT/OT and was discharged to a skilled nursing facility.
Discussion: ODS is a well-known clinical entity associated with rapid correction of hyponatremia. Patients can have progressive neurological symptoms such as bilateral weakness and can also experience dysarthria and dysphagia. Commonly, ODS has been associated with overcorrection of hyponatremia, chronic liver disease, and chronic alcohol usage. Rarely, it can be seen in patients with HHS. In the few case reports of ODS related to HHS, patients demonstrated a similar spectrum of neurologic presentations as our patient with presenting blood glucose levels typically greater than 1,000 mg/dL. Neurologic symptoms in the reports were rapidly progressive and occurred within a day to a week after hospital presentation. In contrast to the pathophysiology of hyponatremia treatment-related ODS in which a too rapid increase in serum osmolarity leads to the sudden shrinking of brain cells (in particular oligodendrocytes), the pathophysiology of ODS in the setting of HHS may be due to the high serum osmolality created by the hyperglycemia itself. This can be seen on MRI brain which will show hyperintense lesions on the T2 weighted MRI. In our patient, she did have a glucose of 1113 mg/dL. Her MRI findings and clinical symptoms are reflective of ODS, and her presentation is most consistent with hyperglycemia as the cause.
Conclusions: Hospitalists should consider ODS on the differential for patients with HHS who start to experience neurological symptoms such as loss of consciousness, loss of sensation and motor function in limbs, dysphagia, or dysarthria without another more apparent cause. Early identification via MRI is important, as it allows initiation of supportive treatments that aide in the recovery of the brain injury.