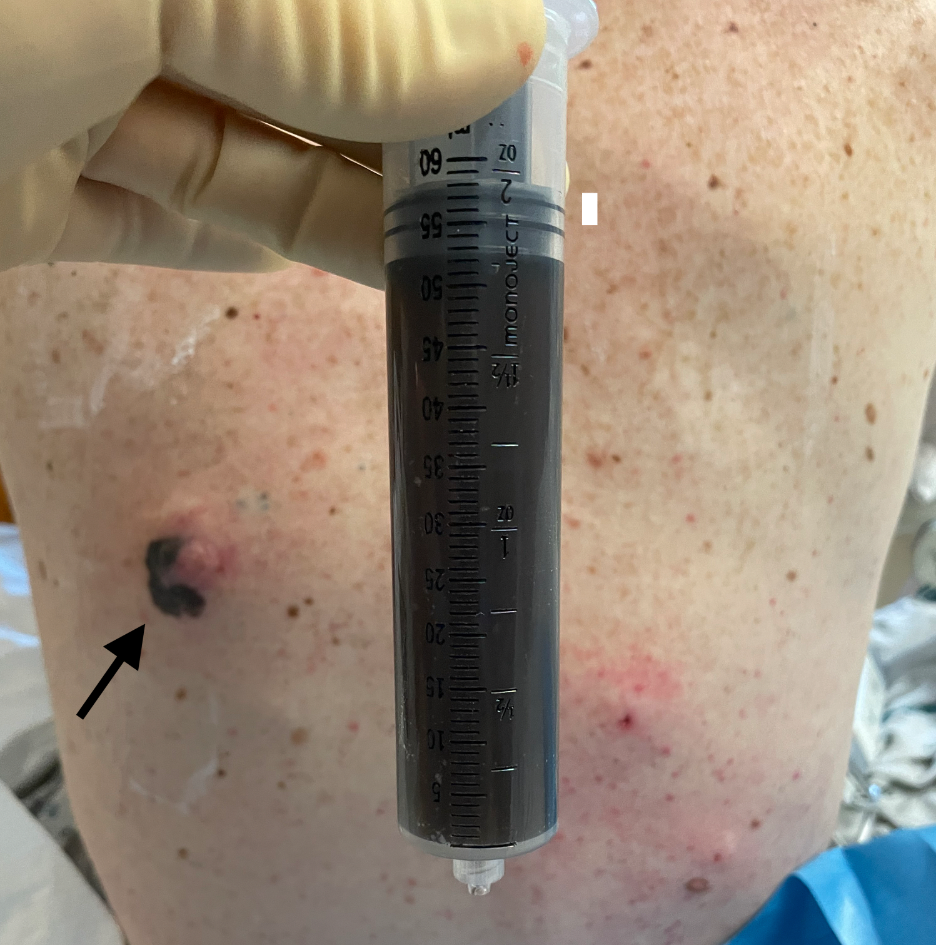
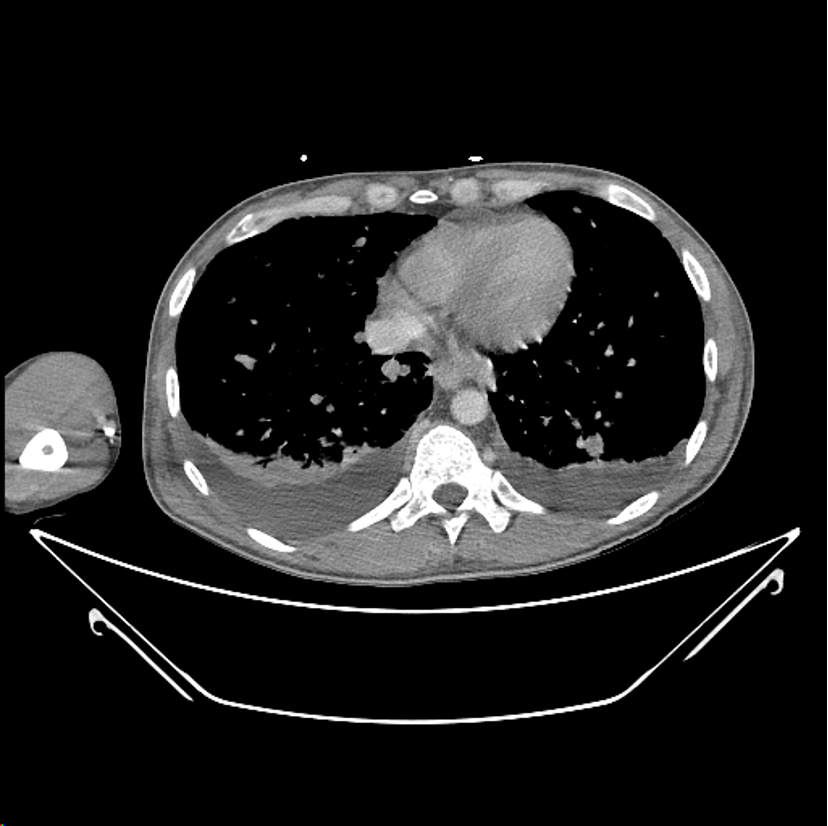
Case Presentation: A 36-year-old man presented with a one-month history of fevers, night sweats, low back pain, and an enlarging nodule on his back. Physical exam revealed left axillary adenopathy, diminished breath sounds at bilateral bases, and an irregularly shaped 10 cm pigmented lesion (image 1) on his left posterior hemithorax. Labs were notable for hypercalcemia (11.1 mg/dL) and a suppressed PTH (3 pg/mL). A CT scan showed diffuse adenopathy, multiple pulmonary and hepatic nodules, small bilateral effusions, and widespread osseous lesions (image 2). A right diagnostic thoracentesis was performed, and 50 mL of black fluid was removed (image 1). Pleural fluid analysis revealed an exudate (pleural fluid LDH 727 U/L, serum LDH 2823 U/L) with 1627 x 10*6 nucleated cells/L with 85% melanoma cells. Cytopathology and molecular testing of the pleural fluid confirmed the diagnosis of metastatic melanoma harboring a BRAF p.V600 mutation. The patient was subsequently started on targeted therapy with binimetinib and encorafenib.
Discussion: Black pleural effusions are rare clinical findings associated with malignancies (melanoma being the most common), fungal infections with Aspergillus niger and Rhizupus oryzae, pancreaticopleural fistulas, hemolysis after intrapleural bleeding, and charcoal containing empyemas (1,2). In the case of melanoma, the black color is due to the cytoplasmic production of melanin by cancer cells (3). While the sensitivity of pleural fluid cytology in diagnosis of malignancy is only around 46% (4), the uncommonly black color of the effusion in this case substantially narrowed the differential diagnosis and allowed for rapid diagnosis without an invasive biopsy.
Conclusions: Black pleural effusions are rare and when discovered, should considerably narrow the differential diagnosis.