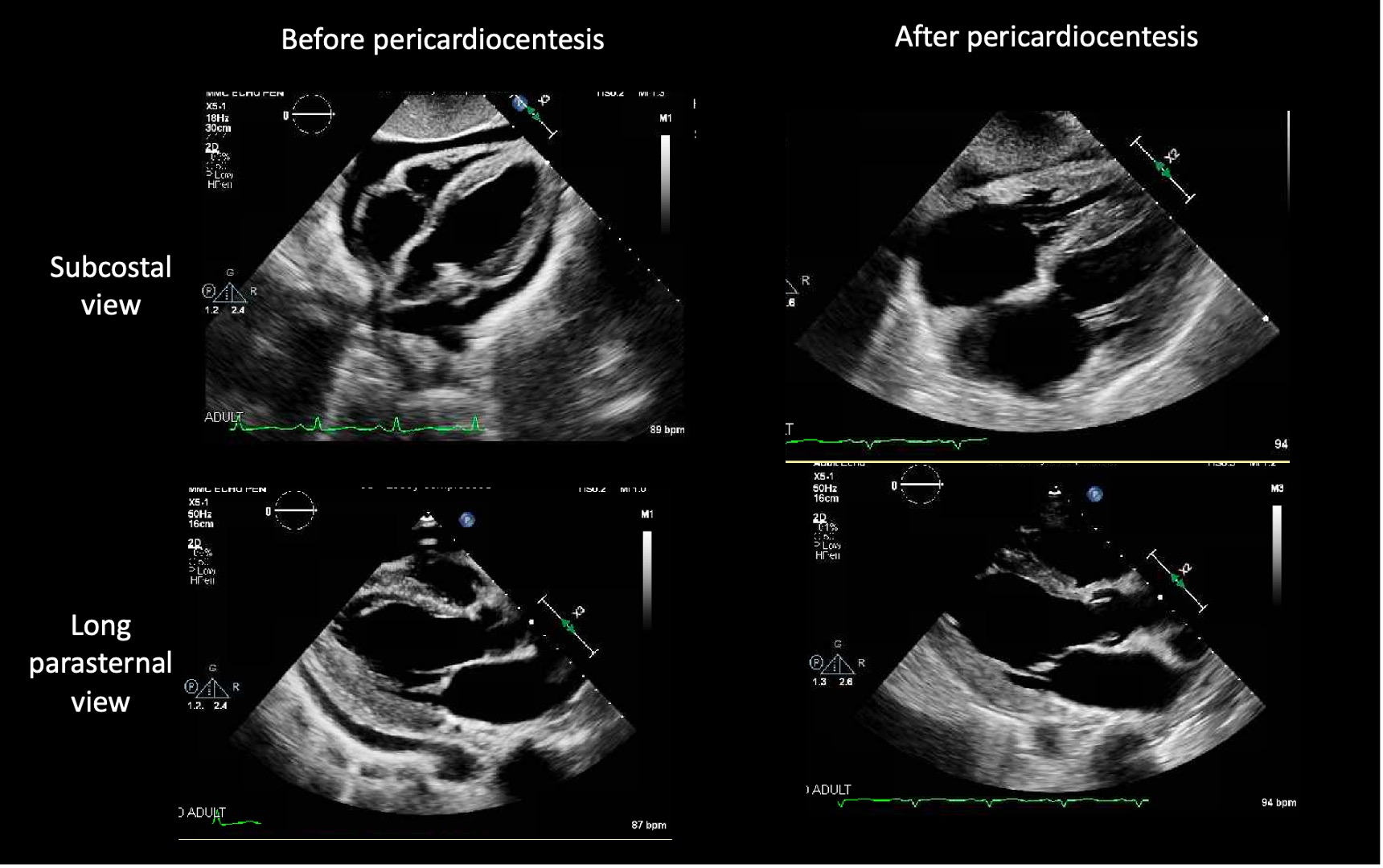
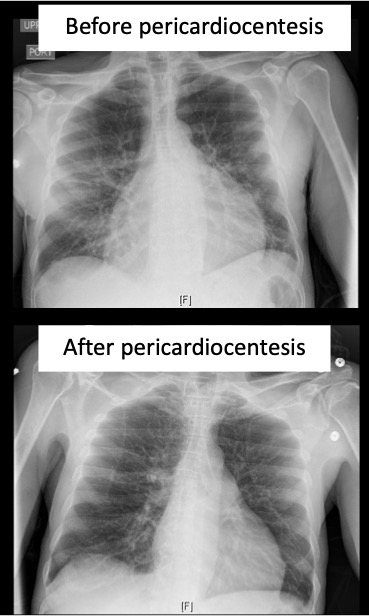
Case Presentation: A 54-year-old- man with past medical history of Acquired immunodeficiency syndrome, recurrent Herpes simplex virus lesion, prurigo nodularis, presented with generalized weakness for one week. On physical examination, diffuse cervical, inguinal and popliteal lymphadenopathy was noted. Echocardiogram showed moderate pericardial effusion, which prompted the patient to undergo emergent pericardiocentesis in the setting of tachycardia, tachypnea, hypotension. The patient’s shortness of breath got improved. Initially, it was assumed that patient had AIDS-related pericardial effusion. Given diffuse lymphadenopathy, urine histoplasmosis antigens were checked, which came back positive. This is an uncommon case presentation of disseminated histoplasmosis-related pericardial effusion. The patient was eventually treated with itraconazole for disseminated histoplasmosis and colchicine for pericardial effusion.
Discussion: Urine and serum Histoplasma antigen are the initial diagnostic workup since it is the most sensitive test for the detection of disseminated histoplasmosis. In one report, antigens were detected in patients with advanced HIV and disseminated histoplasmosis in the following samples: urine (97 percent), blood (83 percent), and CSF (67 percent) [1]. In another study, antigen testing was positive in 39 of 40 patients with HIV in urine and 36 of 37 patients in serum [2]. Liposomal amphotericin B should be used for 1-2 weeks, followed by itraconazole for at least one year until CD4 counts are above 150 cells/mm3, HIV viral load is below 400 copies/mL and Histoplasma urine antigen is negative. Serum itraconazole levels should be monitored to avoid drug toxicity. Antigens should be measured periodically to establish that treatment is effective and to assist in identifying relapse.
Conclusions: Pericardial effusion, a rare manifestation of histoplasmosis, especially in immunocompromised patients, was seen as acute tamponade requiring emergency intervention. The incidence of recurrent disseminated Histoplasmosis related pericardial effusion is low but it must be considered in patients who are in immunocompromised stage and patients who are non-adherent to anti-fungal treatment. These patients should be initiated on corticosteroid and colchicine therapy for histoplasmosis related pericardial effusion.