Background: Ideal care pathways (ICPs) are tools that aim to align clinical practice with evidence-based guidelines through diagnosis-specific standardized care algorithms within the electronic medical record (EMR). Various studies have demonstrated that ICPs are effective in reducing length of stay, in-hospital costs, clinical variation and hospital complications. These benefits, however, are difficult to quantify within a given institution without provider buy-in. Data on successful implementation strategies for ICPs is scarce and more work needs to be done to identify and overcome barriers to provider acceptance and adoption of ICPs into clinical workflow.
Purpose: To increase utilization of ICPs for Heart Failure, Sickle Cell Disease, and Suspected GI Bleed admissions amongst internal medicine residents by at least 10% as part of an institution-wide initiative to increase ICP utilization and improve high-value care.
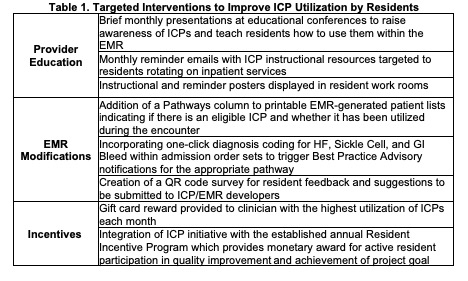
Description: Our institution launched EMR-integrated ICPs for patients admitted with Heart Failure, Sickle Cell Disease, and suspected GI Bleed which together account for thousands of hospital encounters annually. Initial financial data suggests the potential for substantial cost reduction with an estimated savings per encounter of $3,311.08 for Heart Failure admissions and $451.82 for Sickle Cell admissions when the appropriate ICP was opened at least once during the encounter. However, the ICPs are not used regularly, and utilization is particularly low amongst our internal medicine residents with a baseline rate of 3% use for Sickle Cell and GI Bleed encounters and 6% use for Heart Failure encounters (Table 2). Lack of provider awareness and disruption of established EMR workflow were the primary identified barriers to ICP use, thus provider education and EMR modifications were the focus of the implemented interventions outlined in Table 1. Preliminary data after just one month of intervention shows improvement in ICP utilization across all three diagnoses at 26% for Heart Failure, 22% for Sickle Cell and 8% for GI Bleed (Table 2).
Conclusions: Widespread adoption of diagnosis-specific ICPs has the potential to substantially improve the quality, equity and cost-efficiency of patient care delivery in hospital medicine. Regular provider education with reminder systems, incentives, and EMR-modifications to integrate ICPs into previously established clinical workflow appear to be effective ICP implementation strategies.