Background: Peer consultation – the wisdom from collaborating clinicians – is associated with more accurate diagnosis. Programs that provide second opinions or diagnostic time-outs (also known as cross-checks) are thought to improve diagnosis but have not been applied to hospital medicine services. Data from our multicenter collaborative suggest concerns remain about the time required and colleague perceptions around seeking such input. As part of the 13-site Achieving Diagnostic Excellence through Prevention and Teamwork (ADEPT) collaborative, we designed and piloted an intervention (“ADEPT Diagnostic Cross-Check,” or “DXC”) to facilitate peer second opinion discussions focused on reviewing the diagnostic approach in patients on whom a rapid response (RRT) was called, as 16% of RRTs are associated with a diagnostic error and the patient often remains under the care of the same hospitalist, providing an opportunity to change the plan of care. The goals of the DXC were to 1) provide structured diagnostic reasoning support for hospitalists caring for patients experiencing clinical decompensation, 2) serve as a diagnostic pause, and 3) enhance hospitalists’ skill with diagnostic recalibration.
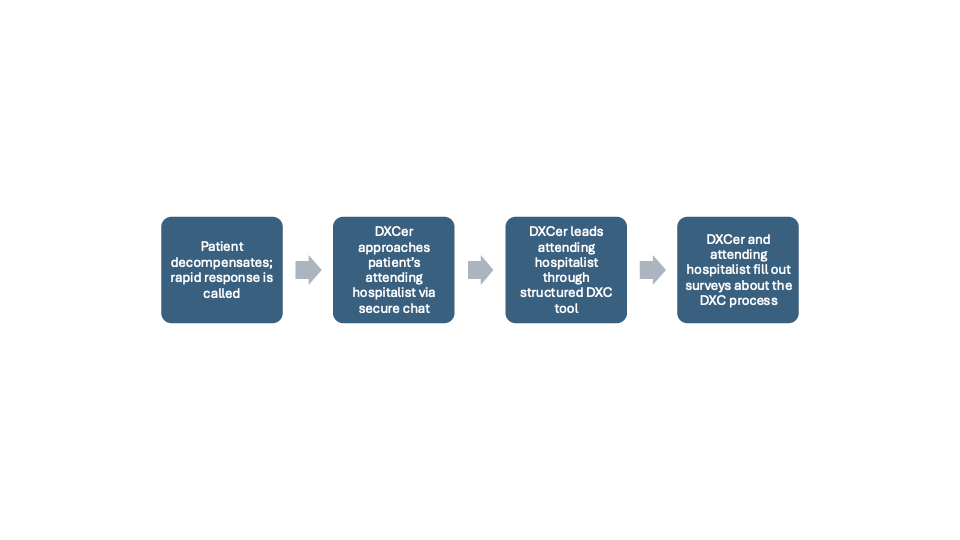
Methods: The DXC program is a peer-to-peer diagnostic collaboration and national pilot study at 13 sites participating in ADEPT for five weeks in August and September 2025. One diagnostic cross-checker (DXCer) was on duty daily, with a goal of performing one DXC per weekday to revisit common diagnostic steps and pitfalls and to identify opportunities to change diagnostic strategy. There were three or four DXCers at each site who were hospitalists participating in the ADEPT collaborative and trained in identifying diagnostic opportunities. DXCers completed training in appreciative inquiry, motivational interviewing, and application to different clinical scenarios using role play of the DXC tool (Figure 1). DXC workflow is delineated in Figure 2.We measured the volume of rapid responses (RRTs) and assessed acceptability (clinician satisfaction and willingness to participate in another cross-check) and value of the DXC (change in care plan for current or future patients) via surveys of the attending hospitalist and the DXCer.
Results: Of the 169 hospitalists approached, 125 (74%) chose to participate in a DXC. Mean DXC duration was 8.6 minutes. 98.8% of clinicians stated they would be willing to participate in a future DXC; 91.8% were satisfied or very satisfied with the process; 37.6% felt participating in the DXC would likely or very likely change the way they cared for future patients; and 15.3% felt the DXC resulted in a care plan change for the discussed patient.
Conclusions: Our pilot results suggest high hospitalist satisfaction with DXCs, which changed the diagnosis in one in seven patients. Current work includes increasing the number of daily DXCs and integrating the cross-checker into clinical roles to foster intervention sustainability. Future work will entail expanding the number of decompensation events included (e.g. including patients with a rising clinical deterioration index), bringing DXCers temporally closer to the clinical decompensation event, and gauging DXC’s effect on fostering a culture of diagnostic excellence.
.jpg)