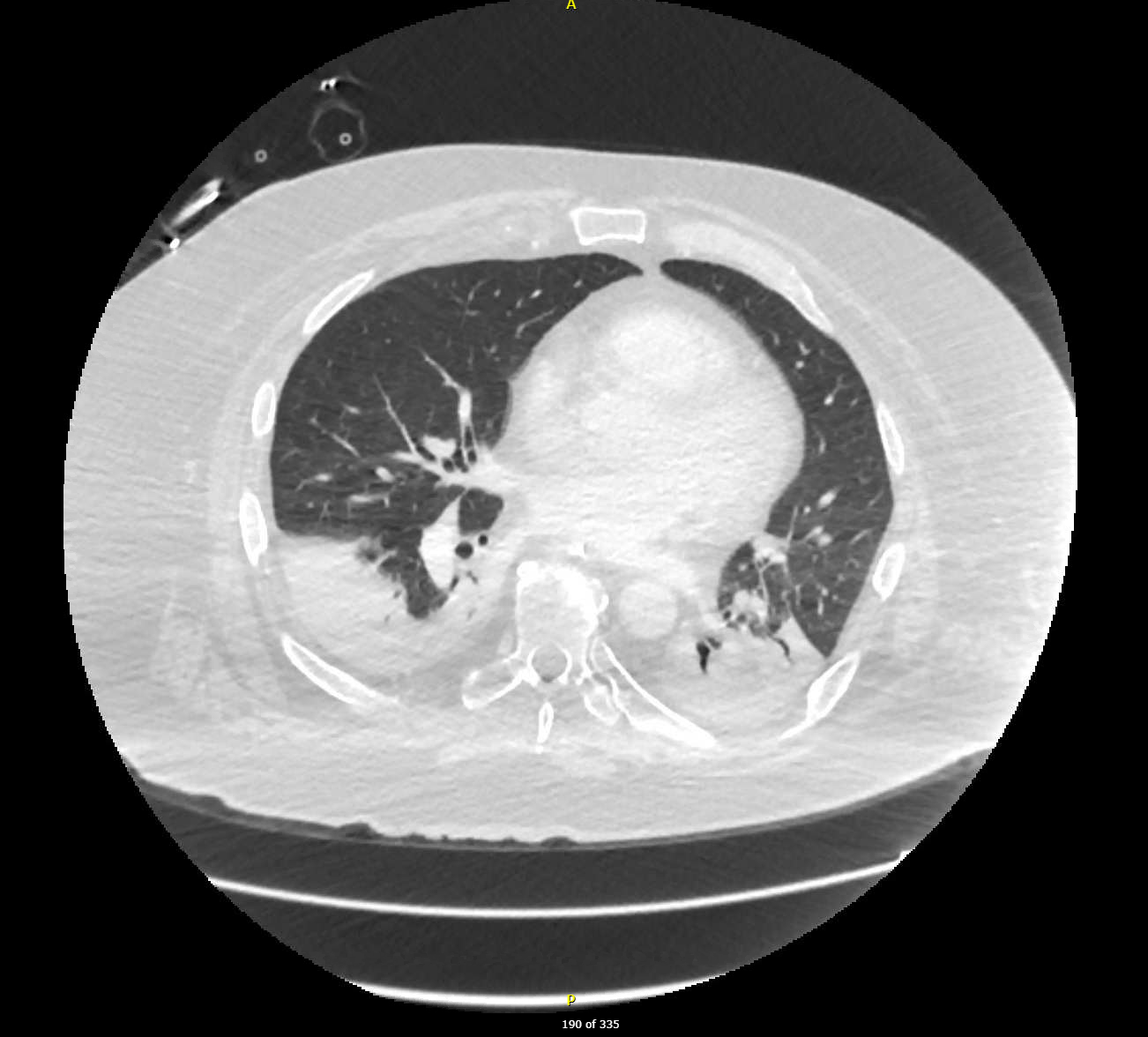
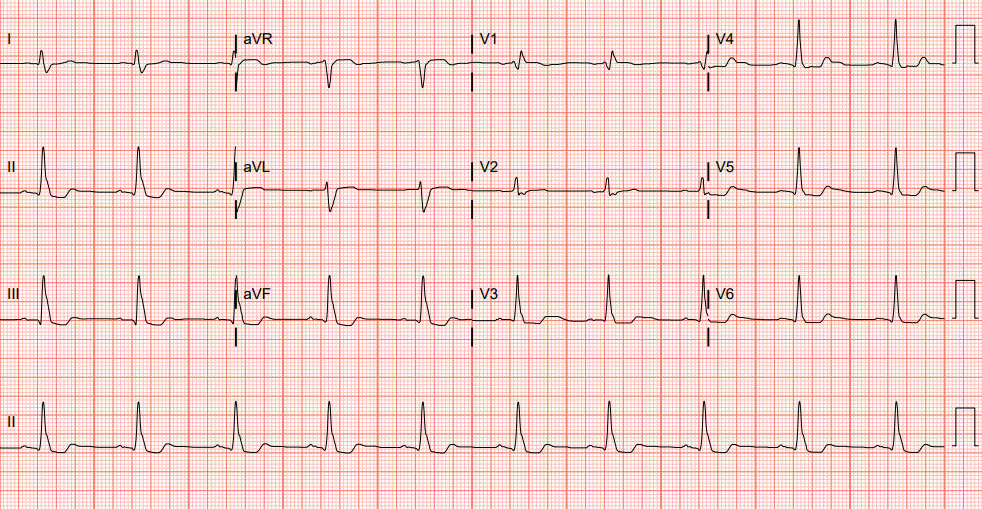
Case Presentation: Our patient is a 68-year-old man with a past medical history of renal cell carcinoma s/p nephrectomy, metastatic melanoma s/p small-bowel resection in 2025 on immune checkpoint inhibitor therapy started 3 weeks prior, and CKD stage III, who presented due to shortness of breath, right-sided ptosis, and worsening bilateral lower extremity edema.In the ER, the patient was hemodynamically stable. Initial labs revealed WBC 11,100, AST/ALT 223/135, HS troponin 440, CK 4,067, aldolase 68.1, and CRP 69.2. Bacterial and viral infectious panels, along with blood cultures, were negative. Further testing showed elevated acetylcholine-receptor antibodies. With the full clinical picture, a diagnosis of Triple M syndrome (TMS) was made. Due to worsening respiratory failure, he was intubated, mechanically ventilated, sedated, and paralyzed. In coordination with Nephrology and Neurocritical Care, he was started on stress dose IV solumedrol and IVIG. With minimal improvement after several days, he then underwent plasmapheresis for 8 days. Despite these measures, the patient’s clinical course worsened due to mixed shock physiology from ventilator-associated pneumonia and NSTEMI.Due to prolonged ventilator requirements, a decision was made in conjunction with the family to perform tracheostomy and PEG tube placement after approximately 14 days. Finally, he received one dose of Rituximab, but unfortunately, he passed shortly thereafter.
Discussion: Immune checkpoint inhibitors (ICIs), such as anti-PD-1 and anti-CTLA-4 therapies, have revolutionized oncologic treatment and are becoming more common, but not without consequences [1]. TMS is estimated to occur in less than 1% of patients receiving these agents, but with reported mortality rates as high as 38% [2].The pathophysiology involves dysregulated immune responses targeting skeletal muscle, heart tissue, and neuromuscular junctions. Clinically, these reactions can result in severe outcomes such as respiratory failure, cardiac arrhythmias, or heart failure, necessitating prompt identification, immunosuppressive treatment, and careful monitoring during ICI therapy to mitigate risks [3].Our patient suffered TMS, induced by a single cycle of ipilimumab and nivolumab for the treatment of metastatic melanoma. Our case highlights management strategies employed by a multi-disciplinary team comprising of Critical Care, Nephrology, and Hematology & Oncology physicians.
Conclusions: Triple M syndrome (TMS), comprising myositis, myasthenia gravis, and myocarditis, is a rare but serious immune-related adverse event increasingly recognized with immune checkpoint inhibitor (ICI) therapy and other medications. Its overlapping clinical features complicate timely diagnosis and require multidisciplinary management.