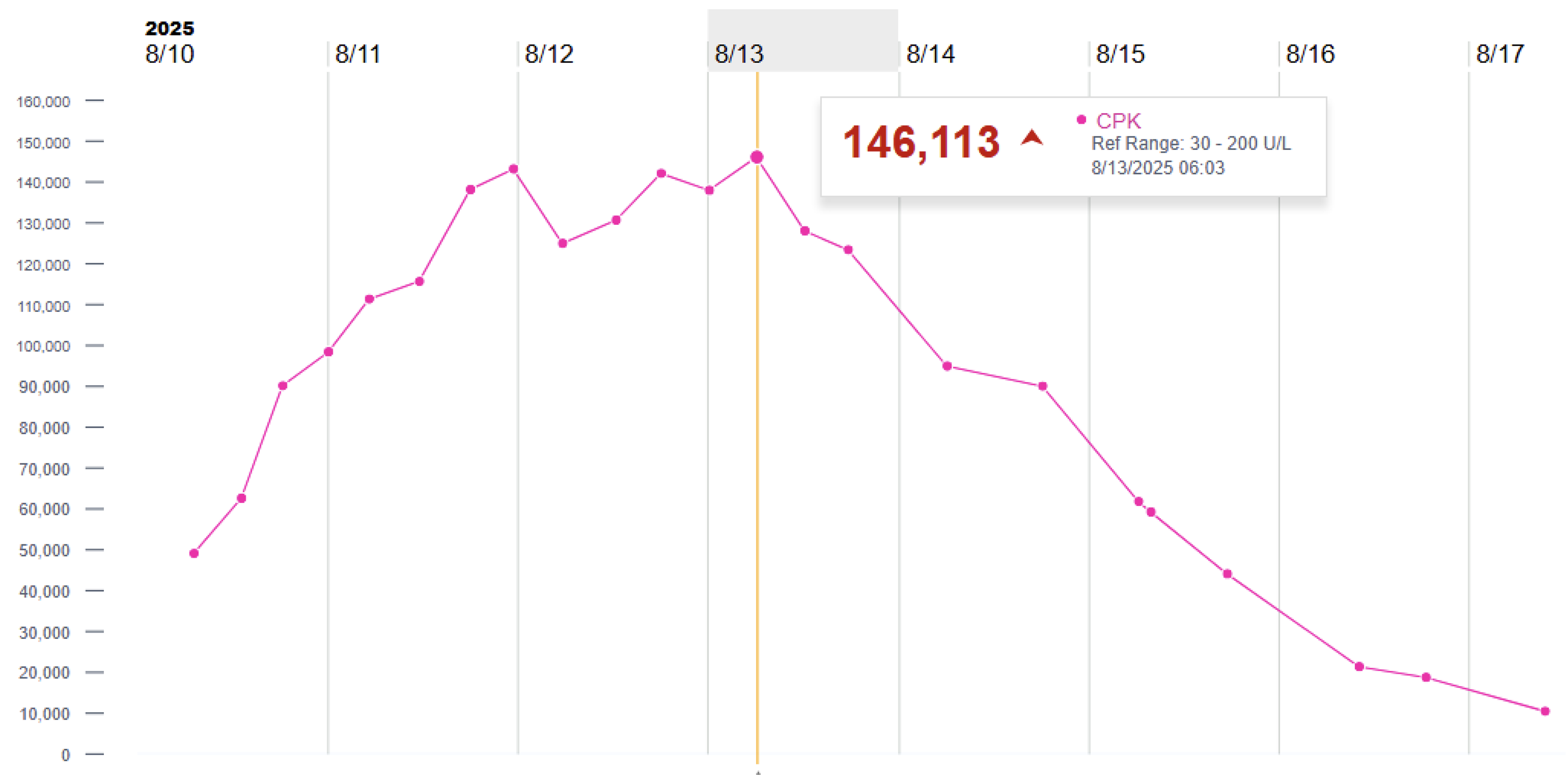
Case Presentation: A previously healthy 16-year-old male presented with six days of headache and abdominal pain followed by three days of fever, myalgias, stiff muscles, nausea, anorexia, and fatigue. He denied exertional activity, trauma, substance use, or recent illness. ED diagnostic evaluation revealed leukopenia (1.96 ×10³/µL), CD4 count 155/µL, thrombocytopenia (121 ×10³/µL), LDH 1210 U/L, hyponatremia (131 mmol/L), and creatine kinase (CK) >22,000 U/L. Urinalysis showed 3+ blood. Imaging studies were unremarkable. HIV 1/2 antigen/antibody screening was positive, and HIV RNA PCR demonstrated a viral load of 7.23 million copies/mL. Other infectious evaluations, including EBV PCR, CMV, hepatitis B, syphilis, toxoplasmosis, Quantiferon-TB, and gonorrhea/chlamydia, were negative.He was admitted for aggressive intravenous hydration with normal saline and bicarbonate-containing fluids, and initiated on bictegravir/emtricitabine/tenofovir. Despite intervention, his CK values continued rising, peaking at 146,113 U/L on hospital day five. A muscle biopsy showed preserved myofiber architecture without necrosis, inflammation, or degenerative changes. Given the prolonged CK elevation, the patient was initiated on dexamethasone (16 mg IV) per an ongoing pediatric clinical trial protocol (NCT06429982). His clinical course improved rapidly thereafter, and he was discharged on hospital day seven with stable renal function (creatinine 0.6–0.7 mg/dL throughout admission).
Discussion: Rhabdomyolysis is a rare but recognized manifestation of acute HIV infection. While a handful of adult cases are documented, pediatric cases remain exceedingly uncommon, with only two prior adolescent presentations reported in the literature. In these cases, HIV-associated rhabdomyolysis occurred without typical precipitating factors and often before full seroconversion was established. This highlights the importance of considering acute HIV infection in the differential for unexplained rhabdomyolysis in adolescent medicine.This case represents a rare instance of acute HIV infection presenting as severe, persistent rhabdomyolysis in an adolescent. Similar to previously reported pediatric cases, no alternative etiology was identified despite extensive evaluation. The lack of biopsy evidence for myositis supports a potentially reversible inflammatory process associated with acute HIV viremia. Notably, the patient’s CK rose for five days despite optimal hydration but improved quickly after corticosteroid administration. Although steroids are not standard therapy for HIV-associated rhabdomyolysis, emerging pediatric data and isolated case reports suggest possible benefit in immune-mediated muscle injury. This case also reinforces that extremely elevated CK does not invariably lead to acute kidney injury, particularly with early aggressive hydration.
Conclusions: Acute HIV infection should remain an important consideration in adolescents presenting with severe, unexplained rhabdomyolysis. Corticosteroids may represent a promising adjunctive therapy in select cases with persistent inflammation and rising CK despite standard management. Further research is needed to clarify their role in pediatric HIV-associated rhabdomyolysis.