
Background: Staffing shortages can impact a rural hospital’s viability. Nighttime coverage is particularly difficult given limited resources, low patient volumes and high provider costs. A tele-hospitalist coverage model split between multiple sites is one solution to minimize these challenges. After successfully creating a daytime tele-hospitalist program to support two rural hospitals, our group at a large academic medical center expanded tele-hospitalist services to four rural hospitals offering both day and nighttime coverage.
Purpose: To evaluate the performance and impact of a tele-nocturnist care delivery model to rural hospitals.In January 2025, our tele-hospitalist care delivery model expanded and added dedicated tele-nocturnist coverage to support patient care. Hypothesized benefits included improved patient care through stability in staffing and continuity of coverage, a decrease in inpatient transfers given provider experience managing tertiary care level patients, and a reduction in provider expenses at each hospital through cost sharing. This pre/post-intervention study reviews financial, performance, and quality measures associated with the addition of a tele-nocturnist model from January-October 2025.
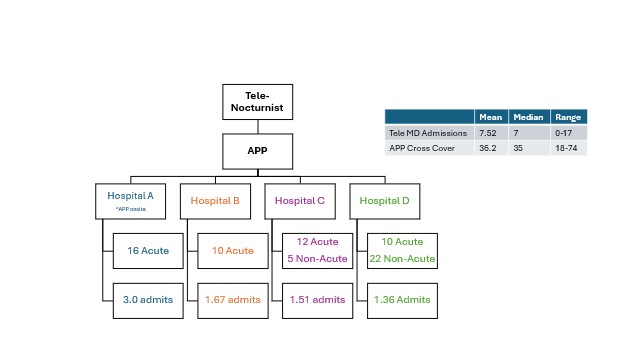
Description: The tele-nocturnist model consists of one physician and one APP performing admissions and cross-cover from 7pm – 7am to four rural hospitals. The virtual physician, supported by mobile carts with Andor video software, is responsible for completion of all new admissions. The APP, located onsite at the highest volume hospital, performs local admissions and cross coverage for patients across all four hospitals (Figure 1). In the first ten months, the tele-nocturnist team has admitted over 2,000 patients (nightly mean= 7.52; median =7, range 0-17), which is approximately 35% of total hospital admissions. The mean number of patients per night under the care of the team is 75, and the mean number of cross-cover pages is 36.2 (median=35, range= 18-74). With readily available provider communication, patient and ancillary staff satisfaction has increased. Per director of nursing at one facility “Having a provider readily available to evaluate and assist with patient care at night has helped to decrease patient care delays and has afforded us the opportunity to proactively treat our patients before their decompensation to a level of care requiring transfer”.With nighttime physician support to the rural hospitals, daytime rounding efficiency is improved as evidenced by an increase in “before 10am discharges” and a decreased length of stay index (Figure 2). Additionally, there was an overall decrease in percentage of inpatients transferred to other facilities and a decrease in mortality compared to previous year (Figure 2).Regarding the financial analysis, the cost of the tele-nocturnist team is shared by the four hospitals which results in greater than ten percent annual provider cost savings (~$25,000), compared to the previous model where each individual hospital pays for an onsite APPs with locum tenens backup.
Conclusions: Our tele-nocturnist care delivery model to support rural hospitals is an example of high value care where we have been able to improve quality at reduced total costs. Having a physician available 24/7 has led to an increase in patient and ancillary staff satisfaction as well as an increase in performance metrics such as LOS index, decreased mortality and reduced transfers. This model serves a long-term viable option for rural nighttime coverage.
.jpg)