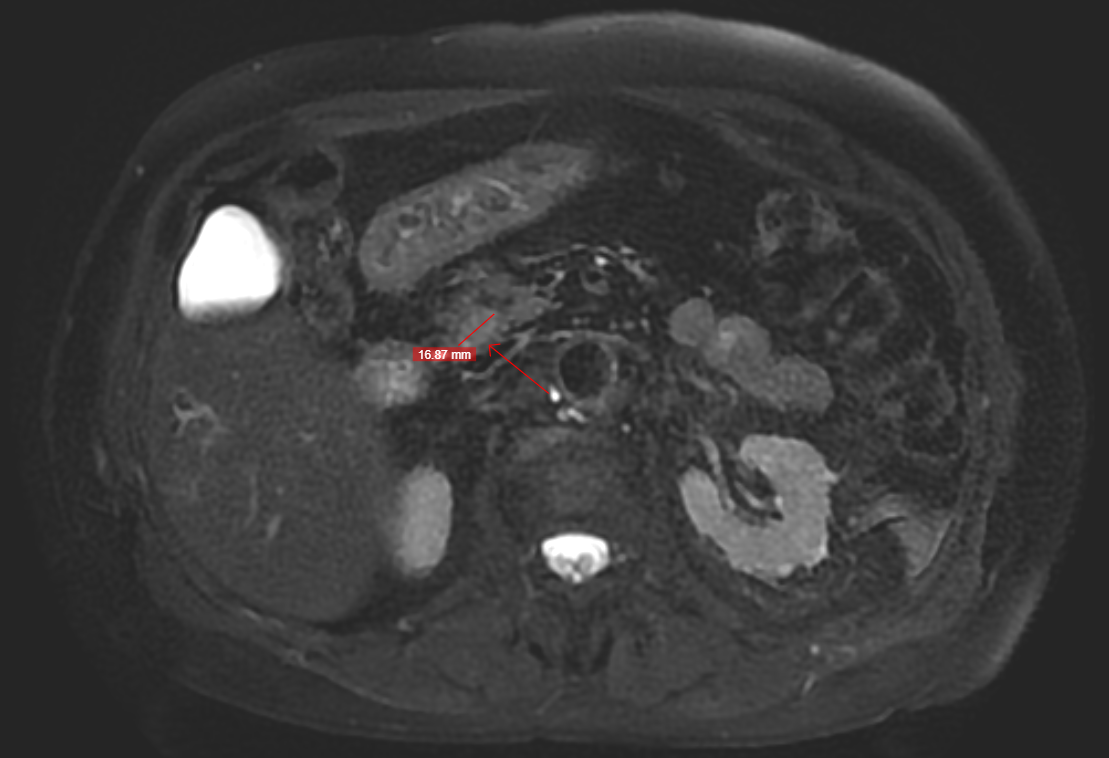
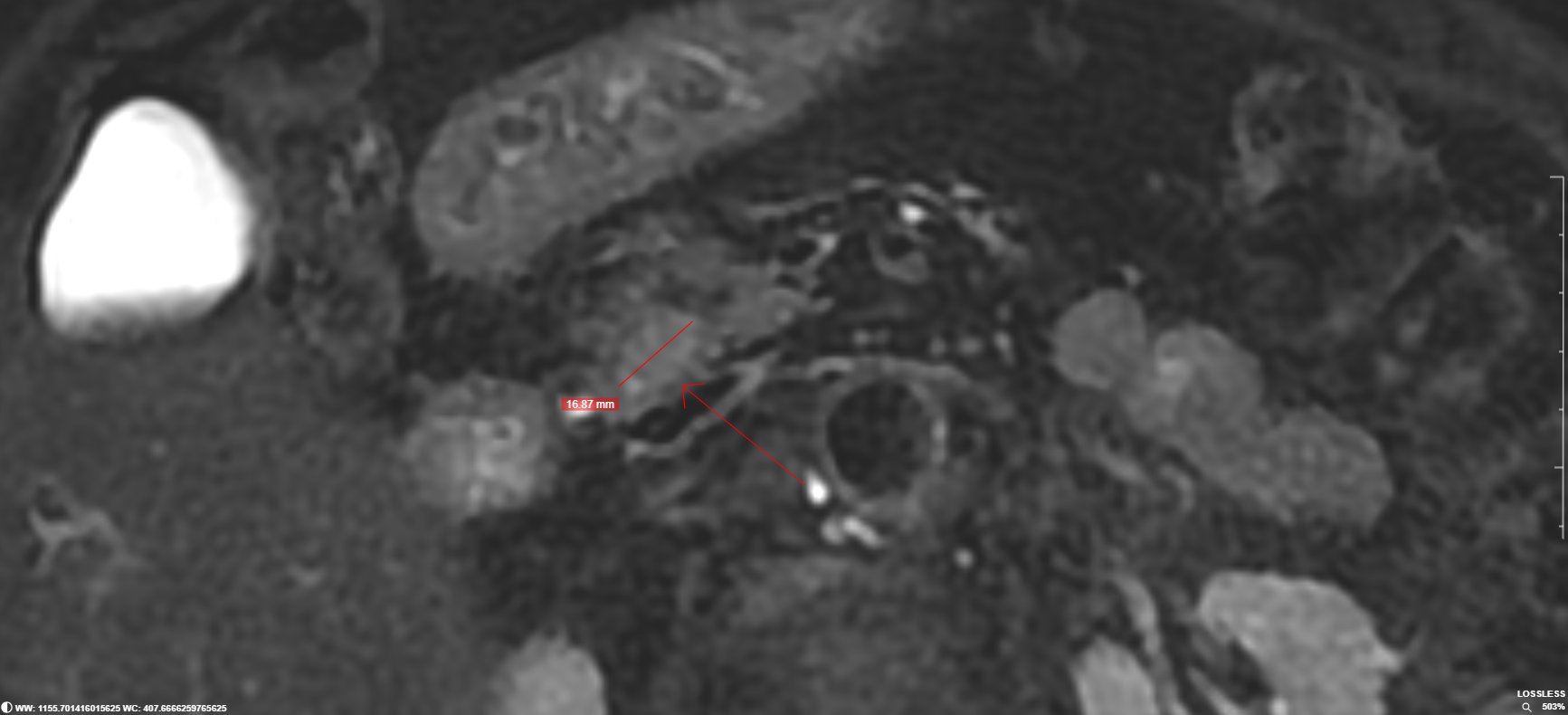
Case Presentation: A 73-year-old woman presented with a 10-year history of recurrent symptomatic hypoglycemia that had intensified over several months. Laboratory evaluation confirmed endogenous hyperinsulinism (serum glucose 57 mg/dL; insulin 32.7 μIU/mL). Contrast-enhanced CT revealed an 18-mm hypervascular nodule in the pancreatic head. MRI and endoscopic ultrasound (EUS) localized a 16-mm well-circumscribed lesion in intimate contact with the main pancreatic duct, without ductal dilation or invasion. Given the lesion’s proximity to critical structures, curative surgery would require pancreaticoduodenectomy, a high-morbidity procedure for this older and medically complex patient. Recognizing this risk, the hospitalist leading her care identified endoscopic ultrasound–guided radiofrequency ablation (EUS-RFA) as a potentially safer, organ-preserving alternative. Although this technique is not part of our national public health system’s procedure catalog, the hospitalist coordinated multidisciplinary evaluation and successfully mobilized the necessary resources for the procedure to be performed in our tertiary hospital. This became the first EUS-RFA treatment for insulinoma at our center. The patient underwent EUS-RFA with concurrent biopsy and without complications. Histopathology confirmed a well-differentiated, grade 1 pancreatic neuroendocrine tumor (Ki-67 < 1%). She experienced complete resolution of hypoglycemia, with capillary glucose levels consistently >70 mg/dL throughout outpatient follow-up.
Discussion: Insulinomas are rare functional pancreatic neuroendocrine tumors and the leading cause of endogenous hyperinsulinemic hypoglycemia. Although the biochemical diagnosis is well established, precise tumor localization can be challenging and often requires multiple imaging modalities and technically demanding procedures for therapeutic planning. While surgical resection remains standard, it may be inappropriate for older adults or patients with lesions in anatomically difficult locations. Lesions abutting the main pancreatic duct often necessitate extensive operations, including pancreaticoduodenectomy, which carries significant perioperative risk. EUS-RFA has emerged as a minimally invasive alternative capable of achieving local tumor control while preserving pancreatic function. Current literature demonstrates high rates of symptom resolution and low complication rates, particularly for well-differentiated, small-volume insulinomas. This case illustrates the applicability of EUS-RFA in a resource-constrained environment, emphasizing the role of hospitalists in recognizing therapeutic options, navigating system barriers, and coordinating multidisciplinary care for complex endocrine conditions.
Conclusions: The complete clinical and biochemical remission observed after EUS-RFA reinforces its potential as an effective, safe, and organ-preserving alternative for insulinomas near vital pancreatic structures, especially in older adults at elevated risk for perioperative morbidity. Beyond the technical success, the case highlights the role of Hospital Medicine: a hospitalist identified high surgical risk, coordinated cross-institutional care, and led an innovative solution despite limited availability in the public health system. This reflects the expanding scope of hospitalists as system-level problem-solvers who improve access to advanced therapies and optimize outcomes for medically complex patients.