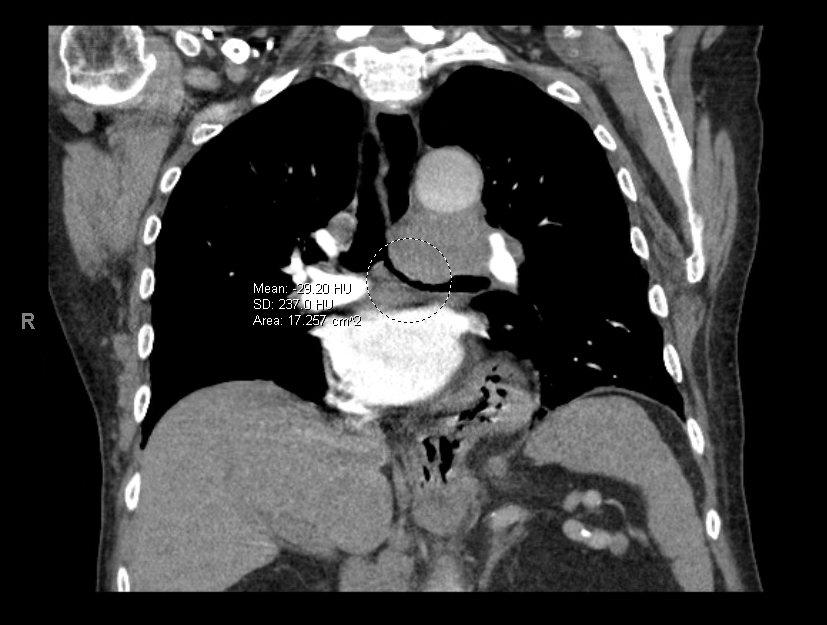
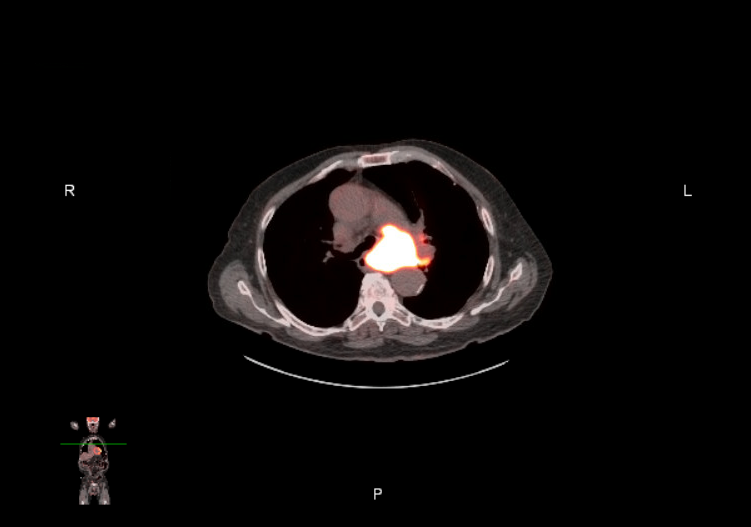
Case Presentation: A 83-year-old male with a history of rheumatoid arthritis on methotrexate and heart failure with reduced ejection fraction (45%) presented with six weeks of progressive dyspnea and dry cough. Chest computed tomography (CT) revealed multiple pulmonary nodules and a large left hilar mass causing complete occlusion of the left main bronchus and left pulmonary artery. Positron emission tomography–CT (PET-CT) demonstrated hypermetabolic activity within the hilar mass and raised concern for a possible tracheoesophageal fistula (TEF). Endobronchial ultrasound (EBUS) with biopsy confirmed Diffuse Large B Cell Lymphoma (DLBCL) invading the esophagus and compressing the left main bronchus with direct visualization of a TEF. Despite this finding, the patient was asymptomatic for dysphagia, regurgitation, aspiration, or recurrent infections. Management options, including upper endoscopy and dual stenting, were discussed, but the patient deferred endoscopic evaluation and elected systemic chemotherapy. Given his stability and absence of aspiration symptoms, he began systemic therapy with R-CEOP (rituximab, cyclophosphamide, etoposide, vincristine, prednisone). Five months later, his respiratory symptoms had significantly improved, and he remained without swallowing dysfunction.
Discussion: TEFs are abnormal connections between the trachea and esophagus that typically present with recurrent infections, aspiration, and malnutrition. In adults, they are usually acquired and malignancy-related, with esophageal squamous cell carcinoma and small cell or non–small cell lung cancer accounting for majority of cases. TEF as an initial manifestation of diffuse large B-cell lymphoma (DLBCL) is exceedingly rare, with fewer than 10 cases reported. When lymphoma causes a TEF, it typically results from chemotherapy-related necrosis in bulky mediastinal disease rather than direct invasion at diagnosis, making this case unusual. Due to the chemosensitivity of DLBCL, lymphoma-associated TEFs may resolve with systemic therapy alone, and several reports describe favorable outcomes without the need for stenting. Conservative management with chemotherapy and close monitoring is appropriate for small or asymptomatic TEFs, while stenting or surgical repair is reserved patients with aspiration, recurrent infections, or worsening symptoms. Upper endoscopy can further characterize TEFs and guide intervention, though individualized decisions are required when patients decline this evaluation, as in this case. For such patients, close follow-up with readiness to repeat bronchoscopy or endoscopy if symptoms evolve is reasonable. This patient’s improvement without stenting is consistent with prior reports of successful conservative management in lymphoma-associated TEFs.
Conclusions: This case highlights the importance of recognizing tracheoesophageal fistula as a rare but clinically significant manifestation of DLBCL. While TEFs from solid tumors often require stenting or surgical intervention, lymphoma-associated TEFs may respond to systemic therapy alone, allowing for a conservative approach in stable, asymptomatic patients. Close inpatient and outpatient monitoring is necessary to detect signs of aspiration, infection, or progression. For hospitalists, early identification, aspiration risk mitigation, and timely coordination with pulmonology, gastroenterology, and oncology can safely guide treatment decisions as well as optimize outcomes.