Case Presentation: A 69-year-old man with severe aortic stenosis (AS), heart failure with reduced ejection fraction, and end-stage renal disease on hemodialysis presented to the ICU after cardiac arrest. Four weeks earlier, he had undergone transcatheter aortic valve replacement (TAVR) with a 29 mm prosthetic valve following balloon valvuloplasty. The procedure was uneventful, and he was discharged on dual antiplatelet therapy.During a routine dialysis session, he developed dizziness followed by monomorphic ventricular tachycardia which led to cardiac arrest. After successful defibrillation and intubation, he was started on amiodarone and norepinephrine. On ICU admission, he had a wide pulse pressure (BP 120/30 mmHg) and elevated troponin (500 → 4356 ng/L), lactate (9.6 mmol/L), and transaminases (>5000 U/L). Echocardiography revealed an ejection fraction of 25–30% with a well-seated prosthetic valve but revealed continuous Doppler flow between the aortic root and right ventricle, raising suspicion for an aorto-right ventricular fistula (ARVF). Transesophageal echocardiography confirmed a 6 mm ARVF.Despite mechanical ventilation, vasopressors, and antibiotics for aspiration pneumonia, the patient’s hemodynamic instability worsened. He was transferred to a tertiary center and was planned for percutaneous intervention for fistula closure using an Amplatzer plug, but his condition rapidly deteriorated, and he expired before the procedure.
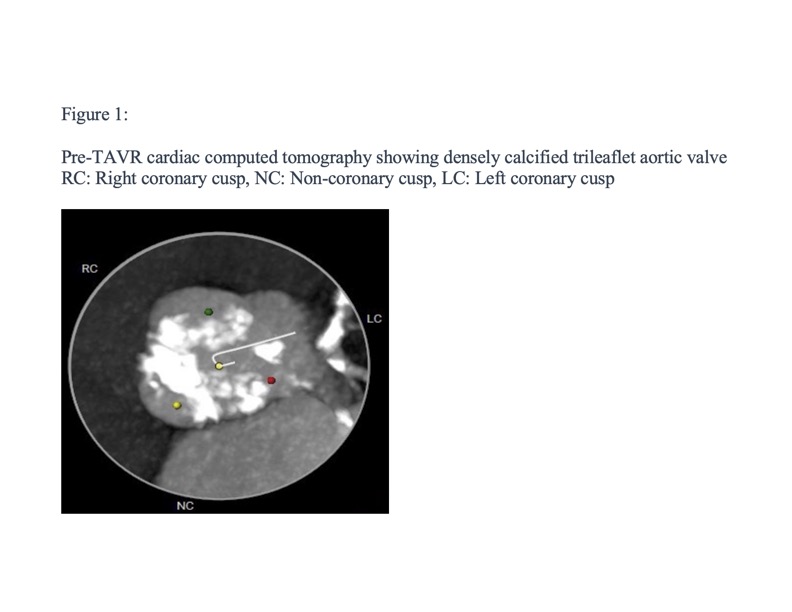
Discussion: ARVFs are rare but potentially fatal complications of TAVR. They result from a tear between the high-pressure aorta and low-pressure right ventricle, often associated with heavy annular calcification or balloon valvuloplasty. The patient’s densely calcified annulus, particularly near the right coronary cusp (Figure 1), likely predisposed to mechanical injury and fistula formation.This case is, to our knowledge, the first reported instance of ARVF after TAVR presenting as cardiac arrest. The fistula produced a left-to-right shunt, reducing systemic vascular resistance thus lowering diastolic pressure, impairing coronary perfusion, and triggering ventricular arrhythmia. Post-dialysis hypovolemia further reduced coronary blood flow, contributing to arrest and refractory hypotension.
Conclusions: As TAVR use continues to expand, hospitalists increasingly care for post-procedural patients. Although ARVFs are extremely rare, they are life-threatening and may present subtly with wide pulse pressure or hemodynamic instability. Awareness of this complication is critical for early recognition, timely echocardiographic evaluation, and prompt referral for intervention. Educating hospitalists about ARVF can improve diagnosis and potentially prevent fatal outcomes in the growing post-TAVR population.